Effects of Melatonin-Rich Milk on Mild Insomnia Symptoms
Article information
Abstract
Background and Objective
Insomnia symptoms are common in the general population. This study evaluated the effects of melatonin-rich milk, which contains 10 times more melatonin than usual milk, on insomnia symptoms.
Methods
Double-blind randomized placebo-controlled trial was performed. A total of 91 subjects aged 21−69 years with mild insomnia symptoms were recruited from the community. All the subjects underwent baseline studies for insomnia severity index, Pittsburgh sleep questionnaire index, Epworth sleepiness scale (ESS), Beck depression inventory and a sleep satisfaction scale (range 1−10). For two weeks, the subjects consumed a cup of either melatonin-rich milk or usual milk before going to sleep. Two weeks later, they completed the same questionnaires used in the baseline. Changes in the questionnaire scores for each group were calculated, after which we compared the differences between the two groups.
Results
Among 91 subjects (male 18, female 73, age 42.1 ± 14.1 years), 44 subjects drank the melatonin-rich milk and 47 drank the usual milk. There was no statistical difference in demographic variables between the two groups. Subjects consuming the melatonin-rich milk reported an improvement in sleep satisfaction scale than the usual milk group (p = 0.023), with significant improvement observed in the subjects aged 20−30 years (p = 0.048). In the ESS Scale, the subjects who had daytime sleepiness showed significant improvement difference between the two groups (p = 0.014), especially in the 20−30 years age group (p = 0.031).
Conclusion
sMelatonin-rich milk could be an easy and beneficial regimen for young people suffering from mild insomnia, by preventing the development of chronic insomnia.
INTRODUCTION
Although several studies report the prevalence of insomnia in the general population, varies from 10 to 48%, there is no controversy that insomnia is a relatively common disorder [1-3]. It is reported that insomnia belongs to chronic disorders, and 45% of patients suffer from its symptoms for over 10 years [4].
According to the insomnia disorder criteria of DSM-5, sleep disturbances alone are not necessarily a diagnosis of insomnia disorder. One third of the general population suffers from sleep disturbances, 10–15% have daytime dysfunction, and only 6–10% meet the criteria for insomnia disorder [1]. It is assumed that approximately 23–27% of the general population have symptoms of insomnia, but do not meet the criteria of insomnia disorder. In other words, 1/4 of the general population who suffers from sleep disturbance is not attended by clinicians. It has been indicated that an inefficient approach to temporary or mild sleep disturbance increases the risk of aggravating to chronic insomnia [5]. It is documented that chronic insomnia is a risk factor of depression, anxiety and alcohol dependence [6-8], and is associated with hypertension, diabetes mellitus and metabolic disorders [9,10]. Daytime sleepiness, known to be related with non-restorative sleep, is also associated with the onset of cognitive dysfunction and dementia [11,12]. Thus, earlier detection and intervention for patients with mild insomnia symptoms is necessary, considering the psychiatric and physical ramifications of chronic insomnia.
Melatonin is a non-sedating hormone secreted from the pineal gland in the brain and has an important role in regulating the sleep-wake cycle. It is synthesized and released only during the period of darkness, from sundown to sunrise. Melatonin in serum prevents awakening, by maintaining a low body temperature and inducing sleep onset [13]. In a study among the elderly population who presented low efficacy of sleep because of low serum melatonin levels, the group consuming 0.3 mg melatonin resulted in normalized serum melatonin levels, and significantly improved sleep efficacy [14]. However, no significant difference was observed between groups consuming 0.3 mg melatonin and 3.0 mg melatonin, which is known to be the inducing pharmacological serum level. Higher serum melatonin levels were reported in the group who took 3.0 mg melatonin. Thus, consuming higher doses of melatonin than required would induce undesirable side effects. Another study, reported that in an elderly population who consumed melatonin-rich milk containing 10 times higher melatonin (10–40 ng/L, 0.5 L) than usual milk, there was a significant improvement in daytime activity without corresponding increase in serum melatonin or decreased core body temperature. Thus, it was concluded that improved sleep quality due to consumption of melatonin-rich milk induced improved daytime activity [15]. Considering that consuming 0.1–0.3 mg melatonin is needed for normalizing serum melatonin level at night, the melatonin level required in melatonin-rich milk is pretty low.
The current study hypothesized that people experiencing mild insomnia, defined as having insomnia symptoms but not meeting the criteria of insomnia disorder according to DSM-5, would require lesser amount of melatonin as compared to those suffering from insomnia disorder. The present study was conducted to determine whether melatonin-rich milk improves the symptoms of mild insomnia beyond the effects of normal milk.
METHODS
Sample
Subjects between 21–69 years age, suffering from mild insomnia but not meeting the criteria of insomnia disorder in DSM-5, were enrolled for this study. Exclusion criteria included illiteracy, psychiatric disorders, medical diseases, or sleep disorders such as sleep apnea and restless legs syndrome. Participants were recruited from 2014.5.26 to 2015.4.30, through notification at the Seoul National University Bundang Hospital and internet advertisement. A total of 91 subjects were enrolled for the study. Approval was obtained from the Institutional Review Board at Seoul National University Bundang Hospital (Reg. no.: B-1403/242−004), and all participants gave informed consent prior to commencement of the study.
Milk Powder
Melatonin-rich milk (CJ Night Milk®, hydrolyzed nonfat dry milk, 12.5 g/sachet) contains 1 ng/sachet melatonin and 58.24 mg/sachet tryptophan. Usual milk (general hydrolyzed nonfat dry milk, 12.5 g/sachet) contains 0.1 ng/sachet melatonin and 46.895 mg/sachet tryptophan. Both melatonin-rich milk and usual milk were procured from the same farm. Subjects were instructed to take the milk powder with warm water (45–50°C), 30 minutes prior to bedtime, each night for 2 weeks.
Study Design
The current study was performed as a double-blind randomized placebo-controlled trial over a period of 2 weeks. Three days before taking the first milk powder, all subjects visited the study center for screening. All participants were evaluated for demographic factors, vital signs, past medical history, and any current medication treatment (Fig. 1). The subjects were all required to maintain a sleep diary. On the first day of the study protocol, all participants visited the study center, and were randomly divided into two groups as melatonin-rich milk group and usual milk group. They were evaluated for vital signs and life style screening, and wrote their sleep-related scales in the sleep diary. All subjects were supplied with their respective milk powder for the 2 weeks study. Participants were required to visit the study center on the 12th day after taking milk powder, with their completed sleep diaries. After completion of 14 days consumption of milk powder, all participants visited the study center on the 15th day, for evaluating vital signs, life style screening, and sleep-related scales. Sleep-related scales in the current study included insomnia severity index (ISI), Pittsburgh sleep quality index (PSQI), Epworth slepiness scale (ESS), and Beck depression inventory (BDI). In addition to Sleep-related scales, the sleep diary accomplished in evaluating subjective sleep satisfaction.
Summary of the study process.
Sleep-Related Scales
Insomnia severity index
The ISI includes severity of sleep onset and maintenance difficulties, satisfaction with current sleep pattern, interference with daily functioning, appearance of impairment attributed to the sleep problem, and the degree of concern caused by insomnia. Each item is scored by the five-point Likert Scale (0 = not at all, 4 = extremely). Score range is 0–28, and total score is classified as follows: 0–7, no clinical significant insomnia; 8–14, subthreshold insomnia; 15–21, clinical insomnia of moderate severity; and 21–28, severe clinical insomnia.
Pittsburgh sleep quality index
The PSQI measures the retrospective sleep quality and disturbances. Individual self-report items assess a broad range of domains associated with sleep quality, including usual sleep wake patterns, duration of sleep, sleep latency, the frequency and severity of specific sleep-related problems, and the perceived impact of poor sleep on daytime functioning. This index consists of 19 items, grouped into 7 equally-weighted component scores. The global score ranges from 0–21. Each component scores range from 0–3. Higher global scores indicate poorer sleep quality. A global score > 5 indicates that a subject reports low sleep quality.
Epworth sleepiness scale
The ESS is a self-administered 8-item questionnaire that measures daytime sleepiness. The instrument includes questions requiring the subject to rate, on a scale of 0–3 their daytime sleepiness in eight specific situations that are commonly met in daily life. The specific situations are: sitting and reading, watching TV, sitting inactive in a public place, being a passenger in a car for an hour, lying down in the afternoon, sitting and talking to someone, sitting quietly after lunch, and stopping for a few minutes in traffic while driving. Global score > 10 indicates that a subject needs to consult a sleep medicine specialist for his daytime sleepiness.
Sleep diary
Sleep diary was used for evaluating the subjective opinion of the participant with regards to sleep. It consists of sleep induction time, waking time, subjective satisfaction, fragmentation, and nap duration.
Beck depression inventory
The BDI is a 21-item, self-report rating inventory that measures characteristic attitudes and symptoms of depression. Each item scores ranges from 0–3. The global score is classified as follows: 10-15, mild depression; 16–23, moderate depression; 24–63, severe depression. Insomnia is a frequently associated symptom of depression or other psychiatric disorders. Hence, the subject’s depression symptoms were evaluated as a potential confounder.
Statistical Analysis
The numbers, percentage, average and standard deviation were presented for the demographic factor and variables of participants. We performed Kolmogorov-Smirnov test for evaluating normal distribution. For analyzing difference of demographic factors between melatonin-rich milk group and usual milk group, we performed the chi-square test for categorical variables, and t-test or Mann Whitney U test for continuous variables, after considering the standard normal variations. For analyzing difference of outcomes between 2 groups, t-test or Mann Whitney U test was conducted, considering standard normal variation. Wilcoxon Signed Ranks Test was planned for comparing pre-test outcomes and post-test outcomes. Statistical analyses were performed with the IBM SPSS Statistics 20 (SPSS Inc., Chicago, IL, USA). p < 0.05 was considered statistically significant.
RESULTS
Clinical Characteristics
Except 3 subjects who withdrew consent, 91 subjects were divided into case group (melatonin-rich milk, n = 44) and control group (usual milk, n = 47). There was no standard normal variation in clinical characteristics of subjects, and hence Man Whitney U test and chi-square test were performed for analysis. Analysis revealed no significant difference in age, sex, marital status, smoking, education year, BMI, SBP and DBP between the two groups (Table 1).

Demographic characteristics
Outcome Analysis
The improvement of insomnia symptoms was analyzed by pre- and post- difference of ISI, PSQI, ESS, BDI, and sleep satisfaction from sleep diary (Table 2). Sleep diaries revealed significant improvement of sleep satisfaction after consumption of melatonin-rich milk (p < 0.001), with significant difference of improvement in melatonin-rich milk group compared to usual milk group (p = 0.023). Although a significant difference was observed in pre-treatment scores between melatonin-rich milk group and usual milk group (p = 0.005) in the ESS, no significant improvement, or difference in improvement, were observed between melatonin-rich milk group and usual milk group. Although significant improvement after consuming milk was observed, there was no significant difference of improvement in melatonin-rich milk group compared to usual milk group in ISI, PSQI, and BDI.
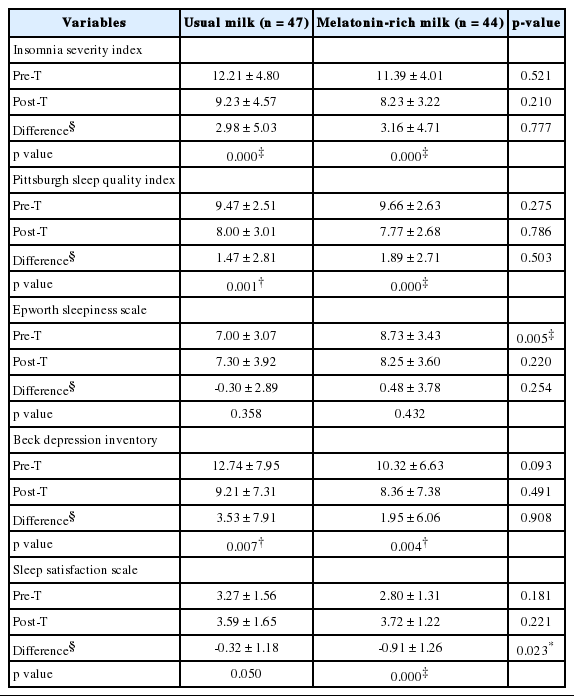
Outcome variables
Analysis as Symptom Severity and Age
In sleep satisfaction from sleep diary, there was significant improvement in melatonin-rich milk group (p = 0.008) and significant difference of improvement in melatonin-rich milk group compared to usual milk group in the age group 20–30 yrs (p = 0.048). There was no significant difference of improvement between two groups in 40–50 yrs and 60 yrs (Table 3).
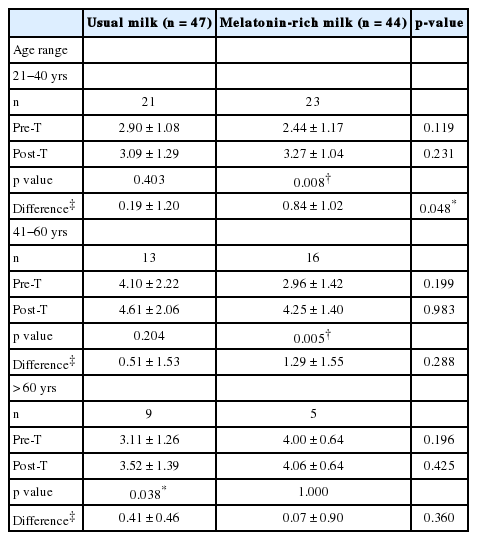
Sleep satisfaction scale analysis
We analyzed the improvement of insomnia symptoms as symptom severity in ESS. There was no significant improvement in the normal group. However, the subgroup suffering from considerable daytime sleepiness showed significant improvement of symptoms (p = 0.003) and significant difference of improvement between normal group and considerable daytime sleepiness group (p = 0.014). Analyzing by age subgroup in ESS, significant difference of improvement was seen in the 20–30 yrs group (p = 0.031) (Table 4). There was no significant difference of improvement in ISI, PSQI, BDI as symptom severity and age.
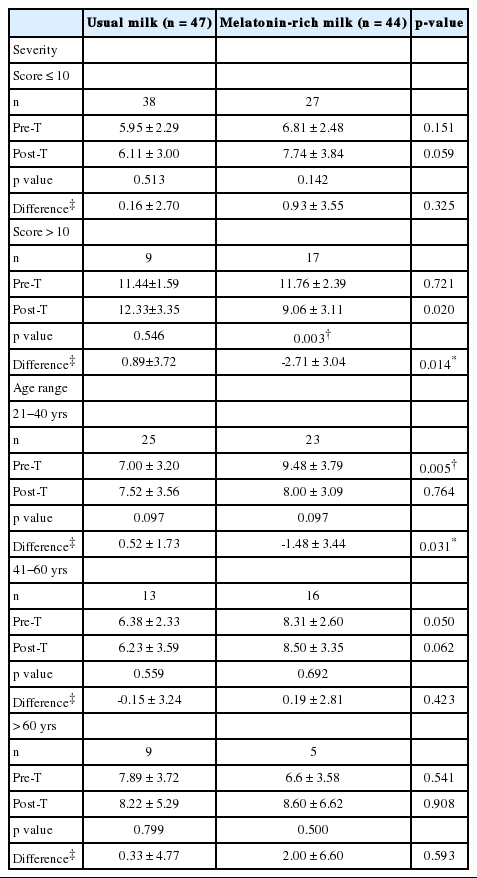
Epworth sleepiness scale analysis
DISCUSSION
According to the current study results, the melatonin-rich milk group showed significant difference of improvement in sleep satisfaction, as indicated from the sleep diary, compared to usual milk group. Analyzing the subgroups by age in sleep satisfaction from sleep diary, there was significant difference of improvement in melatonin-rich milk group compared to usual milk group in the 20–30 yrs subjects. Significant difference of improvement in melatonin-rich milk group compared to usual milk group was observed among those who suffered from problematic daytime sleepiness according to ESS. Results also indicated that there was significant difference of improvement in melatonin-rich milk group compared to usual milk group in the 20–30 yrs subgroup, in ESS. Significant improvement was also noted between pre-treatment and post-treatment in both melatonin-rich milk group and usual milk group, but no significant difference of improvement was seen between melatonin-rich milk group and usual milk group in ISI, PSQI and BDI.
Traditionally, milk is considered to have sleep promoting effect. Two hypotheses are considered for understanding the sleep promoting effect. First hypothesis states that drinking milk reminds an individual of the experience of infancy, where sleep was psychologically induced by breast milk. Second hypothesis is that tryptophan in milk has a positive effect on sleep [16]. It was reported that tryptophan promoted a feeling of relief, and sleep was induced by metabolizing to serotonin and melatonin. Melatonin is a hormone which has a role in the sleep-waking regulation [17]. Our current study was performed to evaluate the effect of melatonin-rich milk, which contained 10 times more melatonin than usual milk, even though the quantity of melatonin is lower than the therapeutic dosage. Usual milk contains 46.9 mg of tryptophan per 1 bag, whereas melatonin-rich milk contains 58.24 mg of tryptophan, a precursor of melatonin. The quantity of tryptophan is higher than the quantity of melatonin (melatonin-rich milk, 58.24 mg of tryptophan, 1ng of melatonin). Because of the high amount of tryptophan in both samples of milk, it is understandable to finding that not only melatonin-rich milk, but also usual milk effects the improvement of sleep.
Reports show that 25% of the general population suffer from non-satisfied sleep, but only 13% of this population visited clinicians, and the critical factor for starting treatment is daytime fatigue [2]. Daytime fatigue and daytime sleepiness can be quite different concepts, but we considered these two symptoms to be positioned in a similar spectrum for subjective experience. According to the results of our current study, there was significant improvement difference between melatonin-rich milk group and usual milk group in daytime sleepiness. Thus, the population suffering from daytime fatigue and daytime sleepiness as mild insomnia symptoms, could be improved by consuming melatonin-rich milk instead of taking sleeping pills.
Previous studies report the incidence of chronic insomnia varies from 9.5% to 10% [18]. There have been many reports about socioeconomic loss, including traffic accidents, due to chronic insomnia [19-22]. The strongest predictable factors for developing chronic insomnia were subjective unsatisfied sleep and other combined psychiatric disorders [5]. The population who suffered from both subjective non-satisfied sleep and combined other psychiatric disorders has a higher risk of developing chronic insomnia, 2 times more than the normal population. Sleep induction time, total sleep time, and numbers of fragmentation during night sleep were not predictable factors of developing chronic insomnia. Also, the risk of developing chronic insomnia was higher in the 20–35 yrs age group, rather than > 65 yrs old population. Reports indicated that the population suffering from clinically noticeable chronic insomnia typically experienced subjective unsatisfied sleep before the onset of chronic insomnia [23], and early detection and intervention of subjective unsatisfied sleep is an effective way to prevent the development of chronic insomnia, especially in the younger population [5]. Results from our current study shows that consuming melatonin-rich milk significantly has a positive effect on daytime sleepiness and subjective sleep satisfaction, especially in the 20–30 yrs group. Thus, consuming melatonin-rich milk prevents development of chronic insomnia in the younger population who experience subjective unsatisfied sleep.
The novel finding of this study was that consuming melatonin-rich milk showed significant improvement difference in ESS and subjective sleep satisfaction only in the 20–30 yrs age group. Explaining the positive effect of melatonin-rich milk in the younger population, some studies were of the opinion that elderly people suffer from insomnia because of lack of decreased level of serum melatonin level and reduction of melatonin receptor [24,25]. A study has reported the reduction of melatonin receptor density in the brain of old rats, and documented recovery of melatonin receptor density after feeding water containing melatonin for 30 days [26]. In another study, elderly insomnia patients were administered 2 mg melatonin for 3 weeks. No significant sleep improvement was observed 1 week later. However, after 3 weeks, significant sleep improvement was observed, as compared to the control group [27]. It was reported that there was significant improvement difference between the two groups which had taken melatonin for 1 week and 8 weeks each [28]. This study indicates that the elderly need more time for improvement of receptor sensitivity, by recovery of melatonin receptors. Hence, time taken for improvement of sleep compared to the younger population would be longer. The results of the present study are similar to the findings from the earlier studies. In the current study, milk consumption was limited to 2 weeks, which is sufficient duration for recovery for younger subjects, but not for the elderly.
The limitation of the current study is that control group was consuming usual milk. As mentioned earlier, usual milk has its own positive effects for sleep. Thus, there is a possibility for underestimating the effects of melatonin-rich milk. Since a longer time is required for improving sleep of elderly people, the duration of the study was quite short i.e., only 2 weeks. If the study period is extended, we may find significant improvement of sleep in the older population. The outcomes of the current study are based on reported scale, and further objective measurements (such as wrist actigraph) can evaluate more reliable results. Further research could compensate all these limitations.
In conclusion, our current study suggests a way to prevent the onset of chronic insomnia in the younger population suffering from mild insomnia. The clinical implication of this study emphasizes the importance of early detection of mild insomnia, and intervention through non-medication by consumption of melatonin-rich milk.
Acknowledgements
This study was supported by CJ®.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.