Comparative Analysis of Pupillometry in Idiopathic Rapid Eye Movement Sleep Behavior Disorder and Parkinson’s Disease
Article information

Abstract
Background and Objective
Pupillary light reflex (PLR) abnormalities have been reported in patients with Parkinson’s disease (PD). However, few studies have been conducted on the abnormality of PLR in patients with idiopathic rapid eye movement sleep behavior disorder (iRBD), which is a prodromal stage of α-synucleinopathy. We herein quantitatively analyzed the PLR of iRBD using an automated pupillometer, and compared the results with those of PD.
Methods
In this cross-sectional study, we prospectively enrolled 27 patients with polysomnography-confirmed iRBD, and 23 patients with PD. Pupillometry was performed three times in each eye, alternating left and right. We compared seven pupillometric parameters between the iRBD and PD patients.
Results
Maximum and minimum pupil diameters were significantly larger in PD patients than in iRBD patients. However, the other pupillometric parameters, such as mean constriction velocity, maximum constriction velocity, reflex amplitude, latency, and mean dilation velocity, did not differ between the two groups. Among iRBD patients, the pupillometric parameters were not correlated with any clinical characteristics related to autonomic dysfunction or neurodegeneration.
Conclusion
s We found that the pupillary constriction and dilation in response to light of iRBD were not different from those of PD. These findings suggest that autonomic pupillary dysfunction already existed in the prodromal stage of α-synucleinopathy to a degree comparable to that in PD. Larger pupil diameters in PD than in iRBD may reflect the pharmacological effect of dopaminergic medications. Future studies are needed to elucidate the association between the PLR abnormalities and the risk of phenoconversion in iRBD.
INTRODUCTION
Rapid eye movement sleep behavior disorder (RBD) is a parasomnia characterized by abnormal motor behaviors, vocalization, and unpleasant dreams during REM sleep [1]. Idiopathic or isolated RBD (iRBD) is defined as RBD that is not associated with any secondary cause, such as neurodegenerative diseases, narcolepsy, or antidepressants. It has great clinical significance, because most patients with iRBD eventually progress to neurodegenerative α-synucleinopathy, such as Parkinson’s disease (PD), dementia with Lewy bodies, and multiple system atrophy [2]. Therefore, iRBD is established as a prodromal stage of α-synucleinopathy, in which dementia or parkinsonism has not yet developed.
Autonomic dysfunction is one of the nonmotor symptoms of PD, and iRBD patients also has a higher frequency of autonomic symptoms, particularly in the gastrointestinal, cardiovascular, and urinary domains, than the control group [3]. Autonomic dysfunction is known to be a major risk factor for neurodegeneration in patients with iRBD [4]. Constipation, urinary dysfunction, erectile dysfunction, and orthostatic hypotension occurred early in the prodromal stage, approximately 6–16 years prior to phenoconversion [5]. This is supported by the results of studies in which α-synuclein inclusions originate in the enteric nervous system, and propagate to the brain through sympathetic and parasympathetic nerves [6,7].
The pupil size changes to control the amount of light entering the eye. Pupillary light reflex (PLR) refers to the pupil constriction in response to light, which is mediated by the parasympathetic innervation to the sphincter pupillae muscle. On the other hand, when it is dark, the pupil dilates by the sympathetic innervation to dilator pupillae muscle. Therefore, the PLR can be used as a clinical diagnostic tool for autonomic nervous system dysfunction. It is possible to quantitatively measure PLR in a fast and non-invasive way using a pupillometer. PLR abnormalities, such as decreased constriction velocity, acceleration, and amplitude, have been documented in patients with PD [8]. However, there are still few studies on the abnormality of PLR in patients with iRBD. Only two recent studies have reported altered pupil responses in iRBD [9,10]. Therefore, we herein quantitatively analyzed the PLR of iRBD patients using an automated pupillometer, and compared the measurements with those of PD patients.
METHODS
Participants
In this cross-sectional study, we prospectively enrolled 27 patients with iRBD, and 23 patients with PD, aged between 50 and 80 years. All patients were recruited from the Department of Neurology at Seoul National University Hospital, and underwent quantitative pupillometry from September 2020 to October 2021. The inclusion criteria in iRBD were: 1) diagnosis of RBD confirmed using video-polysomnography according to the guidelines of the third edition of the International Classification of Sleep Disorders; 2) absence of overt neurodegenerative diseases or other secondary causes of RBD. The inclusion criteria in PD were: 1) diagnosis of PD according to the Movement Disorder Society clinical diagnostic criteria for PD [11]; 2) the Hoehn and Yahr scale measurements between 1 and 2. The common exclusion criteria were: 1) history of orbital trauma, ophthalmologic surgery, and other ocular diseases that may affect PLR; 2) history of diabetes; 3) current use of antidepressant, anticholinergics, or amantadine; and 4) failure to complete pupillometry. The study protocol was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (2005-098-1123), and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants in the study.
Pupillometry
We quantitatively analyzed PLR using NPi-200 (NeuroOptics, Irvine, CA, USA), which is an automated monocular infrared pupilometer system. Participants were first dark-adapted for 3 minutes. The light stimulus was delivered at an intensity of 121 microwatts for a duration of 0.8 seconds. The pupil size change was measured at a sampling rate of 30 frames/second for 3 seconds after light stimulation. Pupillometry was performed three times in each eye, alternating left and right at 1-minute intervals. The binocular measurements were averaged for each subject, and the calculated pupillometric parameters were as follows (Fig. 1): 1) maximum pupil diameter before light stimulation (PDmax, mm); 2) minimum pupil diameter after light stimulation (PDmin, mm); 3) reflex amplitude (RA, [PDmax–PDmin] / PDmax × 100, %); 4) mean constriction velocity (CVmean, mm/s); 5) maximum constriction velocity (CVmax, mm/s); 6) latency (from light stimulation to onset of contraction, s); and 7) mean dilation velocity (DVmean, mm/s).
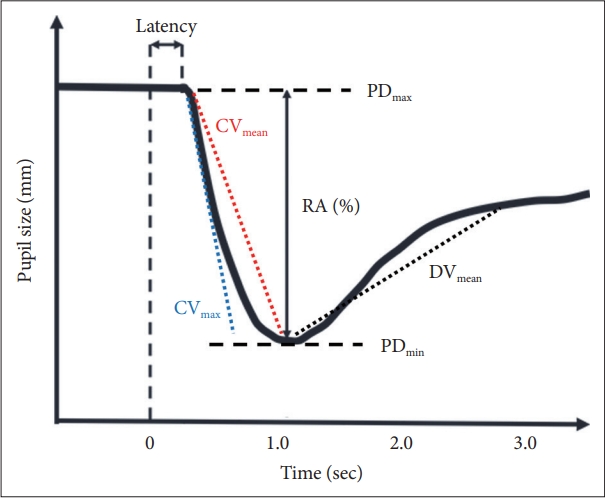
Pupillometric parameters. The vertical line at zero second indicates the onset of light stimulation. PDmax refers to maximum pupil diameter before light stimulation (mm); PDmin refers to minimum pupil diameter after light stimulation (mm); RA is calculated as (PDmax − PDmin) / PDmax × 100 (%); CVmean and CVmax refer to mean and maximum constriction velocity (mm/s), respectively; latency refers to the time from light stimulation to the onset of contraction (s); DVmean refers to mean dilation velocity (mm/s). RA, reflex amplitude.
Clinical Assessments
In both iRBD and PD patients, we investigated the subjective symptoms of autonomic dysfunction using the scales for outcomes in PD for autonomic symptoms (SCOPA-AUT) questionnaire [12]. The Unified Parkinson’s Disease Rating Scale (UPDRS) part III and Hoehn and Yahr scale were used to assess the PD motor symptoms. Current medications for iRBD and PD were also investigated. Levodopa equivalent daily dose in patients with PD was calculated according to conversion factors proposed in a previous study [13]. In patients with iRBD, we further investigated the Korean version of the RBD questionnaire– Hong Kong (RBDQ-KR) [14], the Korean version of Sniffin’ Sticks test II (KVSS II) [15], the Korean version of the Geriatric Depression Scale (GDS–K) [16], orthostatic blood pressure measurement, and the Korean version of Montreal Cognitive Assessment (MoCA–K). RBD is a well-known nonmotor manifestation of PD, and approximately 30% to 50% of PD patients have RBD [17]. Therefore, we evaluated the presence of probable RBD in the PD patients using the Korean version of the RBD screening questionnaire (RBDSQ–K). Probable RBD was defined as the RBDSQ–K of ≥ 5 [18].
Statistical Analyses
Continuous variables, such as the pupillometric parameters, were tested for the assumption of normality using the Kolmogorov–Smirnov test. Then for comparison between the two groups, we used the Student t-test or Mann–Whitney U test, as appropriate. The chi-square test or Fisher’s exact test was used to compare the distribution of categorical variables. In patients with iRBD, the Spearman’s correlation coefficient was used to evaluate the relationship between the pupillometry measurements and clinical characteristics. The statistical significance was defined as a two-tailed probability value of p < 0.05. All statistical analyses were carried out using SPSS software (version 24, IBM Corp., Armonk, NY, USA).
RESULTS
A total of 27 patients with iRBD (mean age, 66.8 ± 7.3 years; men, 48.1%) and 23 patients with PD (mean age, 64.8 ± 6.7 years; men, 60.9%) were included in this study. Age, gender, and education level did not differ between the two groups. Among the iRBD patients, the mean RBDQ-KR score was 34.3 ± 14.4, and 20 (74.1%) were taking clonazepam and/or melatonin, while none were taking dopaminergic agents. Twenty (74.1%) patients had a history of physical injury during sleep. In the PD group, all patients were taking PD medications with a levodopa equivalent daily dose of 303.5 ± 207.5 mg. Eight (34.8%) were found to have probable RBD, and only 3 (13.0%) were taking symptomatic medications for RBD. The total SCOPA-AUT score did not differ between the two groups (12.9 ± 6.5 vs. 11.6 ± 4.6, p = 0.762). Table 1 summarizes the demographic and clinical characteristics of the participants.

Demographic and clinical characteristics of the study participants
Pupillometric analyses showed that the maximum and minimum pupil diameters were significantly larger in the PD patients than in the iRBD patients (PD max, 3.4 ± 0.7 vs. 4.0 ± 1.1 mm, p = 0.014; PD min, 2.4 ± 0.4 vs. 2.9 ± 1.0 mm, p = 0.033). However, the other pupillometric parameters, such as CVmean, CVmax, RA, latency, and DVmean, did not differ between the two groups (Table 2).

Pupillometric parameters in patients with iRBD and PD
Next, we performed correlation analyses between the pupillometric parameters and clinical characteristics in the patients with iRBD. Autonomic dysfunction and RBD symptoms measured by SCOPA-AUT, orthostatic blood pressure drop, and RBDQ-KR score were not correlated with any pupillometric parameters. Potential predictors of conversion to α-synucleinopathy, such as UPDRS part III, KVSS II, GDS–K, and MoCA–K, were also not correlated with any pupillometric parameters (Table 3). Moreover, pupillometric parameters were not correlated with the disease duration after diagnosis or period after symptom onset.

Correlation between clinical and pupillometric parameters in patients with iRBD (n = 27)
DISCUSSION
Abnormalities in PLR have been established in patients with PD. In 66 PD patients without clinical symptoms of autonomic dysfunction, constriction velocity, acceleration, and amplitude were significantly decreased, and constriction latency was increased, compared to controls [19]. Furthermore, PD patients with cognitive impairment had more reduced pupillary constriction velocity, acceleration, and amplitude than PD patients without cognitive impairment [20]. However, maximum and minimum pupil size per se did not differ between the PD and control groups. Taken together, the PLR abnormalities in patients with PD are characterized by reduced and slow pupil constriction in response to light, suggesting impairment of the parasympathetic nervous system innervating the sphincter pupillae muscle.
In this study, we examined PLR by using the pupillometer in patients with iRBD and PD. The major pupillometry parameters, such as CVmax, CVmean, RA, latency, and DVmean, did not differ between the two groups, which indicates that iRBD patients already have PLR impairment comparable to that of PD patients. In particular, CVmax, CVmean, RA, and latency are considered to reflect the parasympathetic activity, while DVmean reflects the sympathetic activity during PLR. Our findings are consistent with a recent study by Perkins et al. [9] that demonstrated that pupil constriction and dilatation in iRBD patients were significantly decreased compared to controls, but were not different from those in PD patients. A decrease in pupillary constriction amplitude in patients with iRBD was also found in a chromatic pupillometry study [10]. Notably, only iRBD patients with positive skin biopsy for α-synuclein deposits showed significant PLR abnormalities compared to controls, supporting that parasympathetic pathways are affected by the underlying α-synucleinopathy in iRBD.
Of the 7 pupillometric parameters in this study, the only difference was the larger pupil diameter before and after light stimulation (PDmax and PDmin) in the PD patients, than that in the RBD patients. Larger baseline pupil diameters in patients with iRBD and PD compared to controls were reported in a few studies [10,21]. Along with the reduced constriction amplitude and delayed latency, they are considered to reflect parasympathetic dysfunction. In this regard, our findings can be interpreted as worsening of PLR abnormalities caused by the disease progression from iRBD to PD. However, several studies in patients with PD revealed no significant difference in the baseline pupil diameter, compared with controls [19,22,23]. Moreover, patients with late-stage PD had significantly decreased constriction velocity than patients with early stage, whereas baseline and minimum pupil diameter did not differ according to the disease stage [24]. It should also be considered that dopamine induces pupil dilation by stimulating α-adrenergic receptors at the dilator pupillae muscle. There was a significant dose–response relationship between the baseline pupil diameter and total L–DOPA dose, especially at ≤ 400 mg per day [25]. Therefore, the larger pupil diameters in PD than in RBD may be attributed to the effect of dopaminergic agents, rather than parasympathetic dysfunction caused by the neurodegenerative progression of α-synucleinopathy.
Among iRBD patients, the pupillometric parameters were not correlated with any clinical characteristics related to autonomic dysfunction or neurodegeneration. In agreement with this, there was no significant correlation between pupillometric parameters and presynaptic dopaminergic deficits measured by dopamine transporter imaging in patients with PD [26]. In another study, pupillomotor dysfunction in patients with PD was not associated with the presence of skin denervation, cognitive decline, axial motor impairment, or RBD [27]. These findings indicate that neuropathology causing PLR abnormalities, non-motor symptoms, and motor dysfunction in PD does not occur simultaneously, and their progression rates are heterogeneous. Therefore, no association between the pupillometric parameters and clinical findings in our study can be interpreted as the presence of pupillary autonomic dysfunction in the early stage of prodromal α-synucleinopathy, in which only the lower part of the brain stem is affected, and cognitive impairment, olfactory dysfunction, or mild parkinsonian signs have not yet developed. It is also possible that the self-report questionnaires, such as SCOPA–AUT and RBDQ–KR, did not accurately reflect the severity of autonomic dysfunction and RBD symptoms. Longitudinal observations will be required to determine whether the abnormal pupillometry findings are an early biomarker of neurodegeneration in iRBD.
There are several limitations to this study. Since there was no comparison with healthy controls, it is not completely certain that the pupillometry results in our patients are truly abnormal, although PLR abnormalities in PD and iRBD have been established. Autonomic dysfunction was evaluated only with self-report questionnaires, but was not supported by quantitative autonomic function tests. In addition, the small sample size might have reduced the statistical power to identify differences between the two groups. Further studies comparing iRBD patients with drug-naive PD patients are needed to rule out the effects of dopaminergic medications on the PLR.
In conclusion, we found that pupillary constriction and dilation in response to light of iRBD were not different from those of PD. These findings suggest that autonomic pupillary dysfunction already existed in the prodromal stage of α-synucleinopathy to a degree comparable to that in PD. Larger pupil diameters in PD than in iRBD may reflect the pharmacological effect of dopaminergic medications. Future studies are needed to clarify the role of the PLR abnormalities as a predictor of autonomic dysfunction and phenoconversion in iRBD.
Notes
Availability of Data and Material
Deidentified data are available from the corresponding author upon reasonable request.
Authors’ Contribution
Conceptualization: all authors. Data curation: Jun-Sang Sunwoo. Formal analysis: Jun-Sang Sunwoo. Funding acquisition: Jun-Sang Sunwoo, KiYoung Jung. Investigation: Han-Joon Kim, Ki-Young Jung. Methodology: Jun-Sang Sunwoo. Resources: Han-Joon Kim, Ki-Young Jung. Writing—original draft: all authors. Writing—review & editing: all authors.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
This work was supported by the research fund of the Korean Society of Sleep Medicine, and National Research Foundation of Korea (NRF) grants funded by the Ministry of Science, ICT & Future Planning (2017R1A2B2012280, 2017M3C7A1029485).