Four Useful Concepts When Treating Patients With Insomnia: Possibility of Sleep Index-Based Cognitive Behavioral Therapy for Insomnia
Article information

Abstract
Cognitive behavioral therapy for insomnia (CBT-I) is one of the most common treatments for insomnia and is considered as the first-line treatment. People who struggle to fall asleep or stay asleep or those who do not find sleep refreshing can benefit over four to six sessions of CBT-I. Although CBT-I has many benefits, it does have some drawbacks. Therefore, a brief version needs to be developed for use in clinical practice. This study proposes the following concepts that can be readily applied in clinical practice: 1) Concept 1, 17 hours of activity and 7 hours of sleep; 2) Concept 2, discrepancy between desired time in bed and desired total sleep time; 3) Concept 3, time in bed during 24 hours; and 4) Concept 4, taking sleeping pills 7 hours before the waking up time. These concepts based on sleep indices could easily help patients with insomnia and may serve as a foundation for the development of Sleep Index-based CBT-I.
INTRODUCTION
There is no doubt that insomnia is one of the most common and annoying conditions affecting humans. Sleep disorders, such as insomnia, often lead to other psychiatric disorders. Research has consistently demonstrated a connection between insomnia and numerous medical conditions, such as obesity, diabetes, and cardiovascular diseases, as well as cancers [1]. Due to the inability to fall asleep easily, patients worry about the consequences. The “3P” behavioral model for insomnia [2] suggests that chronic insomnia is primarily perpetuated by poor sleep hygiene, maladaptive behavior, and dysfunctional thinking for sleeping. These dysfunctional beliefs about sleep [3] affect the severity of insomnia. It is common for patients who have dysfunctional beliefs about their insomnia to tend to prefer lying down earlier than one’s previous or regular sleeping time [4]. Furthermore, they usually have maladaptive beliefs and worry about falling asleep, which further leads to sleep-related problems.
Cognitive behavioral therapy for insomnia (CBT-I) is one of the most common treatments for insomnia and is considered as the first-line treatment [5]. This program consists of four to six sessions that can help people who have trouble falling asleep or staying asleep or those who find sleep unrefreshing. Besides teaching the patients specific skills that are useful if insomnia returns later in life, as it often does, this goal-directed therapy also helps them learn coping strategies. The positive effects of CBT-I are long lasting, and most people report increased sleep satisfaction [5]. Nonetheless, despite the numerous benefits of CBT-I, it has some drawbacks, such as being time-consuming (requiring an average of seven face-to-face sessions) and expensive (requiring a specially trained professional therapist). Since it may not always be practical to provide classical CBT-I treatment by a professional therapist, various types of CBT-I models have been developed or used, including a brief version of CBT-I, smartphones-based model, email-based model, online-delivery model, or digital therapeutics-based CBT-I [6]. It is also necessary to develop an easy model that can be applied in the busy environment of clinical practice. This study proposes some concepts that are related to sleep indices (Table 1), which can be readily applied in clinical practice. Additionally, these concepts may serve as a foundation for the development of a sleep index-based CBT-I (SIBT-I).
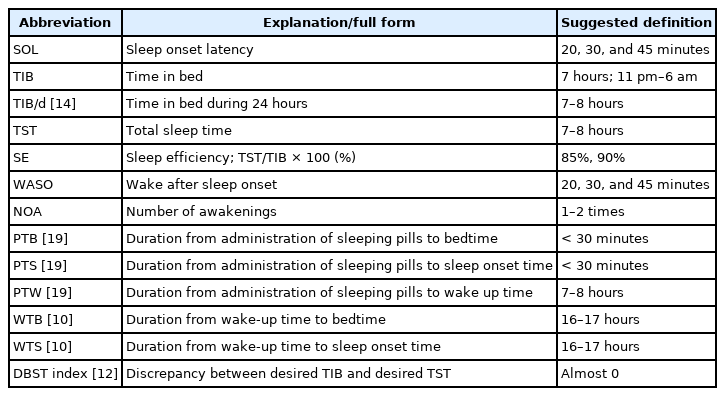
Useful sleep indices applied in clinical practice
CONCEPT 1: 17 HOURS OF ACTIVITY AND 7 HOURS OF SLEEP
While trying to sleep early, insomnia patients cannot fall asleep without a conducive circadian rhythm and the homeostatic pressure to sleep. An average adult needs 7–8 hours of sleep per day [7]. If people take a nap during the day, their “real” sleep time, which is the duration that they slept, would be subtracted from the amount of sleep required. This could be explained by the model of sleep regulation [8] that involves two processes, process S (homeostatic drive) and process C (circadian process). In process S, the longer the period of arousal, the more pressure one feels to sleep. In process C, people sleep according to their circadian rhythm, and the suprachiasmatic nucleus plays a critical role in regulating the circadian rhythm [9].
Based on this two-process model of sleep regulation [8,9], it has been shown that both circadian rhythm (process C) and homeostatic drive (process S) contribute to the quality of sleep. Because circadian rhythm alone is not sufficient for regulating sleep, homeostatic drive as well as the pressure to sleep is required for good sleep. A previous study showed that short sleep latency (SL) was associated with a long duration from wake-up time to bedtime (WTB, 16.5 h in SL ≤ 30 minutes group and 15.8 h in SL > 30 minutes group) [10]. The same study showed a significant correlation between short SL and a long duration of WTB (r = -0.43, p < 0.01). The study results demonstrate that even when circadian rhythm is adequate, it is necessary to sustain wakefulness (homeostatic drive) for good sleep. Therefore, based on these findings, it can be concluded that approximately 17 hours of activity are needed for short SL. A 7 hours of sleep does not guarantee 17 hours of activity, but 17 hours of activity may provide 7 hours of sleep.
CONCEPT 2: DISCREPANCY BETWEEN DESIRED TIME IN BED AND DESIRED TOTAL SLEEP TIME
Usually, people believe that they need at least 6–8 hours of total sleep time (TST) each day. Patients with dysfunctional beliefs about their sleep problem often go to bed early at night with the goal of falling asleep quickly. This may be because they believe that an early bedtime will ensure falling asleep easily. On the other hand, the two-process model suggests that ample wakefulness hours are necessary for falling asleep in a timely manner [8,9]. As described in Concept 1, the two-process model of sleep regulation showed that homeostatic drive (process S) is important for better sleep. Insomnia patients often use the phrase “I would like at least 5–6 hours of sleep,” when they cannot fall asleep easily and maintain their sleep well. This quotation is merely a statement about how desperately they want to sleep well. It is also just one piece of the puzzle of dysfunctional beliefs about sleep. If they want to sleep for at least 6 hours (desired TST) and fall asleep early in the evening, they should wake up early in the morning (6 hours of TST beginning at a bedtime of 10 PM would lead to a wake-up time of 4 AM). However, they may wake-up in the morning around 6–7 AM, which might reduce the sleep efficiency (SE), and hence answer that they want to sleep longer (desired time in bed [TIB]) than the desired TST, when a clinician asks them, “From what time to what time do you want to sleep?” This desired TIB, which is dysfunctionally longer than the desired TST, might decrease the SE. Shortening the TIB is effective in increasing the SE, based on the concept of the sleep restriction technique in CBT-I; hence, this dysfunctionally long desired TIB should be assessed.
As the name suggests, the discrepancy between desired TIB and desired TST index (the DBST index) reflects the discrepancy between one’s desired hours of TIB and desired hours of TST. The concept of this index comes from this dysfunctional thinking regarding their sleep–wake cycle [11]. The desired TST can be determined by asking, “For what number of hours do you wish to sleep per day?” The desired TIB can be determined by asking, “From what time to what time do you wish to sleep?” The DBST index is calculated as “desired TIB hours–desired hours of TST” [12]. According to a previous report [11], the DBST index is one of the components predicting insomnia severity in the general population, along with depression, preoccupation with sleep, and dysfunctional beliefs about sleep. Moreover, a persistent preoccupation with sleep mediates the impact of dysfunctional beliefs about sleep and the DBST on insomnia severity. In cancer patients [13], the DBST index showed a significant correlation with and was a predictor of insomnia severity. Moreover, it had a significant correlation with and was a predictor of SL in those patients. It is necessary to examine the DBST index with sleep parameters obtained from objective nocturnal polysomnography in future studies.
CONCEPT 3: TIME IN BED DURING 24 HOURS
TIB is an important sleep indicator for measuring a person’s sleep–wake pattern. This tool is particularly useful for assessing the sleep–wake cycles in people with circadian rhythm disorders, such as delayed sleep phase syndrome or advanced sleep phase syndrome. When we measure a person’s sleep–wake pattern, we usually consider their bedtime and wake-up times during the night. Patients suffering from severe illnesses, such as paralysis, cancer, or renal failure, or those undergoing hemodialysis easily spend most of their daytime lying down. Notably, cancer-related fatigue might influence sleep disturbance in cancer patients. During CBT-I for cancer patients [14], daytime cancer-related fatigue symptoms are one of the precipitating factors that can influence the perpetuating factors. Therefore, assessing TIB during 24 hours (TIB/d) may help to explore a person’s physical activity during the day [14].
TIB/d can be measured by asking, “What is the average number of hours you spend lying down during 24 hours, regardless of whether you sleep?” A previous study reported that TIB/d was significantly longer in cancer patients with SL > 30 minutes than in those with SL ≤ 30 minutes [15]. However, in another study, a significant correlation between TIB/d and insomnia severity could not be shown [16]. It was speculated that TIB/d, as a possible index for daytime activity, could be a useful index for daytime fatigue symptoms. Further studies are needed to explore the utility of TIB/d as a measure for daytime fatigue symptoms.
CONCEPT 4: TAKING SLEEPING PILLS 7 HOURS BEFORE THE WAKING UP TIME
While CBT-I should be used as a first-line treatment for insomnia, some physicians often prescribe sleeping pills. Most physicians advise their patients to take sleeping pills around 30 minutes before bedtime [17,18], and most patients are aware of this advice. This generally helps patients to sleep, but some complain that they are unable to sleep when using these drugs in this manner. Many patients who are not satisfied with hypnotics seek to increase the dose in order to improve their sleep quality. When patients complain that they are dissatisfied, doctors are more likely to prescribe a higher dose of hypnotics or switch to other medications. Taking multiple medications or higher doses is more likely to increase the risk of falls, daytime somnolence, drowsiness while driving, and drug abuse and dependency. Thus, understanding the reasons for poor therapeutic response to these medications is essential.
According to the two-process model, insomnia patients should go to bed based on their sleep–wake cycle. However, most patients generally take sleeping pills 30 minutes before the time that they desire to go to sleep rather than the time when they should go to sleep based on their sleep–wake cycle. According to a previous research [19], patients who were not satisfied with the sleeping pills (z-drug or benzodiazepine) tended to take them at 09:16 PM and go to bed at 09:47 PM, whereas those who were satisfied tended to take them at 11:11 PM and go to bed at 11:22 PM Patients in both groups consumed sleeping pills within 30 minutes of bedtime, but those who consumed them later at night were generally satisfied with the sleeping pills. Furthermore, patients in both groups fell asleep at similar times (11:31 PM versus 11:45 PM), which suggests that the dissatisfied group stayed awake in bed for a longer period than the satisfied group (104.6 minutes versus 23.4 minutes). In addition, the study also showed that patients who were satisfied with sleeping pills spent 7.1 hours in bed and 7.2 hours until their wake-up time in the morning, whereas patients in the dissatisfied group spent 8.8 hours in bed and 9.3 hours until wake-up time in the morning. Moreover, 85%–96% of the patients were satisfied with their sleeping pills when the time from administration of sleeping pills to wake-up time (PTW) was ≤ 7–8 hours. In contrast, the satisfaction rate was slightly lower (62%) when the time from administration of sleeping pills to bedtime (PTB) was ≤ 30 minutes. According to the results, the recommendation of taking sleeping pills 7–8 hours before getting up might be more effective than the usual recommendation of taking the pills 30 minutes before bedtime.
In another study [20], the possibility of administering sleeping pills 7 hours before the usual wake-up time rather than the conventional consumption 30 minutes before bedtime was investigated. Three-fourths of the participants in this study who were dissatisfied with their hypnotics were satisfied when they consumed their sleeping pills 7 hours before their usual wakeup time. The mean TIB and PTW were significantly shortened and seemed reasonable as no serious side effects were reported. This approach involves concepts of CBT for insomnia and circadian rhythm regulation (delaying the advanced bedtime), since it considers when the patients take the sleeping pills and when they go to bed. Though we should consider various situations and possibility of modification or change the ‘7 hours,’ this method would be easier for doctors to explain to their insomnia patients when they are unfamiliar with the CBT concepts.
DISCUSSION
This study describes the four approaches for managing insomnia in the busy environment of clinical practice. As mentioned before, these concepts are based on sleep indices. Sleep indices are very useful assessment tools. However, they are considered less effective than maintaining a sleep diary for 2 weeks, actigraphy, or nocturnal polysomnography. Before prescribing antihypertensives or oral hypoglycemics, doctors must check the patient’s blood pressure or blood glucose. Similarly, sleeping pills should be prescribed only after checking all sleep indicators, such as the time to go to bed, time to fall asleep, time to get up, and time to wake up. Combining these four time points will give us information on the patient’s sleep–wake cycle, dysfunctionally long TIB, or long SL. Moreover, the time of taking sleeping pills will provide us an insight regarding the administration of sleeping pills in these patients. To better determine the patients’ sleeping pill administration patterns, the use of new sleep indices such as PTB, PTW, and time from administration of sleeping pills to sleep onset was proposed in previous studies [19]. Since subjective satisfaction with sleeping pills was influenced by the time of their administration, it was proposed to instruct the patients to take their sleeping pills 7 hours before their wake-up time [19]. Although it was found that instructing patients to take their sleep medicines 30 minutes before bedtime generally helped decrease sleep disturbances, it may be more beneficial to have them take their sleep medicines at a designated time based on their wake-up time [20].
TIB is a sleep index that can help us identify a patient’s sleep–wake cycle. Furthermore, reversing TIB (WTB, 24 hours–TIB) reveals the patient’s daytime activities [10]. According to the two-process model, an early bedtime does not guarantee an early sleep onset. To sleep for 7 hours, 17 hours of activities must be performed each day. By reversing the TIB, the WTB index will provide an insight regarding the appropriate time to go to bed. Similarly, the TIB/d index also provides information of the patient’s daytime activities. We can measure the patient’s inactivity using TIB/d, but we cannot recognize what they are doing by just measuring TIB during the night. Thus, it is hypothesized that TIB/d can be used to measure the patient’s daytime fatigue symptoms, though it is not easy to measure subjective fatigue symptoms with a relatively objective index. To assess the sleep–wake cycles of patients, such as those with severe illnesses or cancers, TIB/d can be a beneficial index [16].
When conducting CBT-I for patients with insomnia, dysfunctional beliefs about sleep are an important concept to consider. The DBST index seems related to the dysfunctional beliefs about sleep. Our previous studies [11-13] showed a correlation between the DBST index and rating scales for measuring dysfunctional beliefs about sleep. Although the severity of insomnia is the most powerful predictor of the DBST index, dysfunctional beliefs about sleep may also have an effect on it. Even though it is not a sound concept, it can still be used as a single sleep index that can easily assess patients’ dysfunctional beliefs about sleep in a clinical setting.
These concepts have several limitations. First, the concepts have not been fully verified. Several studies were conducted to explore these concepts in the general population or insomnia patients; however, further studies involving other groups, such as cancer patients or shift-workers who may suffer sleep disturbances, are warranted. Second, these concepts should be explored in relation to objective measures such as actigraphy or nocturnal polysomnography. Since the sleep indices are based on the physicians’ questions or sleep diaries maintained in clinical settings, further studies comparing sleep indices with nocturnal polysomnography results are needed. Finally, there is no evidence that sleep indices-based interventions are effective in reducing insomnia in the long term. Long-term follow-up studies need to be conducted to examine the effects of interventions for insomnia based on these concepts.
In conclusion, CBT-I is an important and effective treatment for insomnia. Nonetheless, a brief alternative model is warranted for use in a busy environment in clinical settings. This study proposed to utilize the existing useful sleep indices as well as some more measures that may be useful in clinical practice. These sleep indices could easily help patients with insomnia, and we can develop a new CBT-I model based on sleep indices, SIBT-I.
Notes
Availability of Data and Material
Data sharing not applicable to this article as no datasets were generated or analyzed during the study.
Conflicts of Interest
Seockhoon Chung, a contributing editor of the The Korean Society of Sleep Medicine, was not involved in the editorial evaluation or decision to publish this article.
Funding Statement
None
Acknowledgements
I would like to express my appreciation to all my team members and alumni of the Asan Medical Center sleep and psycho-oncology laboratory who aided me in developing the numerous concepts for diagnosis and management of insomnia, such as the DBST, sleeping pill administration time, or TIB over 24 h.