Chinese Translation and Validation of the Child and Adolescent Sleep Checklist for Parents
Article information

Abstract
Background and Objective
The Child and Adolescent Sleep Checklist (CASC) for parents was originally developed and published in Japanese and has served as a valid and effective tool for the assessment of a parent’s perspective of their adolescent child’s sleep behaviors. To allow for comparisons of such perspectives among parents of different cultures, and with different linguistic backgrounds, reliable and valid measurement tools are necessary. The purpose of this study was to translate and validate a Chinese language version of this questionnaire.
Methods
Internal consistency, factor structure, and criterion validity data were tested using 497 parent/adolescent dyads in Taiwan. Exploratory factor analysis (EFA) and internal consistency reliability were examined in a subset of the cohort (n = 241), while criterion validity and conduct confirmatory factor analysis (CFA) was examined in a second subset of the cohort (n = 256). Preliminary criterion validity was established through a comparison with a measure of chronotype, Morningness-Eveningness Scale for Children.
Results
EFA resulted in four factors, consistent with the original version, with the four factors accounting for 60% of the total variance. The results of CFA presented good fit to the data. The questionnaire demonstrated also acceptable to good internal consistency (α = 0.84–0.89). Preliminary criterion validity was evident as the total score and each of the subscale scores on the questionnaire were significantly higher (worse sleep-related behavior) in evening-types.
Conclusions
The Chinese language version of the CASC for parents appears to be a psychometrically sound measure to evaluate sleep behaviors in Chinese-speaking adolescents.
INTRODUCTION
Worldwide, adolescents are reported to have insufficient sleep [1,2]. Such sleep curtailment is likely due to bedtimes that extend late into the night combined with fixed wake times that are associated with early school start times. The delay in bed time in teens is caused by a combination of both biological (i.e., puberty-associated delay in the timing of the circadian clock) and social factors (e.g., increased socialization, education requirements, entertainment options) [3]. For individuals who are evening-type, the delay may be worse and lead to even shorter sleep durations and greater daytime sleepiness [4,5].
One factor that is involved in the determination of bed timing, which can be readily overlooked, is that of parent involvement [6]. For example, recent adolescent studies have demonstrated that adolescents with parent-set bedtimes on school nights reported earlier bedtimes on school nights, more sleep on school nights, less fatigue, and had less trouble maintaining wakefulness [7]. In a systematic review of children’s sleep, McDowall et al. [8] report that when parents did not recognize that their child’s sleep habits fell outside of societal norms, there was a risk that the child was more likely to report irregular sleep schedules and would not be referred appropriately when they had sleep pathologies. Parent reporting of their child’s sleep is also critical in situations in which the child is unable to report sleep problems [8]. Parent reporting of sleep, however, is likely culturally-specific as what is considered “normal” may vary considerably [9]. As such, it is critical to have valid, language-specific tools.
One of the more commonly used tools to assess sleep behaviors by parents is the Sleep Habits Questionnaire [10], which has been previously translated into Chinese [11]. This tool, however, was designed to assess sleep behaviors among elementary students, not adolescents. The Child and Adolescent Sleep Checklist (CASC) [12,13] was designed to identify sleep habits and screening for sleep problems among both children and adolescents. The CASC has three versions: parent/caregiver (CASC-P), elementary school children (2–11 years of age), and high-school students (12–18 years of age). The different versions of the CASC have good reliability (0.8 to 0.98) [12,13] and internal consistency (Cronbach’s α = 0.79) [14]. The CASC-P, specifically, examines a child’s sleep from the perspective of the parent; it is currently available in Japanese and English.
Given the focus of the CASC-P on parents of adolescents, the lack of an equivalent scale for a Chinese language speaker, and the importance of parental involvement in setting sleep-related behaviors, we thought it important to translate and develop a Chinese version of the CASC-P while establishing the factor structure and internal consistency for the questionnaire. To provide a preliminary criterion validity to this questionnaire, we examined its relationship to chronotype, as adolescents with an evening chronotype have typically been shown to have poorer sleeprelated behaviors [4,15].
METHODS
We recruited adolescents who were enrolled as full-time students in eight different public high schools in northern, central, and southern regions of Taiwan. The students were recruited on the basis of expressing difficulty in initiating sleep early enough or having to wake up too early. Adolescents using medications specifically for sleep disorders were excluded. Questionnaires concerning sleep were given to both the adolescent and at least one parent. All participants (dyads of one parent and one adolescent) signed a consent form prior to participation. The study was approved by the National Cheng Kung University Institutional Review Board (IRB No. A-ER-103-351). All procedures were conducted in accordance with the Declaration of Helsinki.
Translation of the CASC-P
Questionnaire translation
We performed forward (English to Chinese) and backward (Chinese to English) translation to ensure the equivalency of meaning between the original and translated versions. Each translation step was performed by two independent translators [16]. We also invited experts in related fields to ensure the accuracy of the final version. In the forward translation, two native Taiwanese translators with good knowledge of Chinese and sleep-related studies independently translated the CASC-P into a Chinese version. Throughout the translation process, translators were asked to focus on the conceptual equivalence, thereby avoiding a literal translation. Translators were also asked to translate into Chinese words that were natural and acceptable for the broadest range of individuals. Researchers compared the two translations (T1 and T2), discussed them with both of the translators, and then combined them to form a new translated version (T3).
Backward translation
The translating approach for the backward translation was the same as with the forward translation. Two native English speaking translators with sufficient proficiency in Chinese independently translated T3 into an English version. Both back translators had no knowledge of the original, English version of the CASC-P. As with the forward translation, translators were asked to focus on conceptual rather literal equivalence. Researchers compared the two back translations (BT1 and BT2) and discussed them with the two back translators, then combined them to form a new back version (BT3). The Chinese version (T4) was revised according to BT3.
Experts committee
Two bilingual and experienced clinicians who specialized in sleep reviewed the concepts among all translations (T1–T4 and BT1–BT3) and original questionnaire. The clinicians ensured that the final Chinese version was equivalent to the English CASC-P in terms of semantics, culture, and concepts. If the clinicians thought that some items were inappropriate, the researchers would repeat forward and backward translation until the concepts were acceptable. The researchers analyzed the reliability and validity of the final Chinese version.
Research Design and Participants
We used a two-stage research design to analyze the reliability and validity. Stage 1 (n = 241 parents of students in grades 9–12) involved analysis of the internal consistency reliability and exploratory factor analysis (EFA). The sample size fulfilled the EFA’s requirement of 5–10 participants for each of the 24 questions [17]. Stage 2 (n = 256 parent/child dyads of students in grades 9–12) involved analysis of criterion validity (sleep problem differences by chronotype) and confirmatory factor analysis (CFA). The sample size fulfilled the CFA’s requirement of at least 200 participants [18].
Measures
CASC-P
The CASC-P is designed to estimate a parent’s impression of their teenager’s sleep. The CASC-P consists of two sections. The first section (12 items) consists mostly of general questions about the child’s sleep timing; this section is not part of the scoring of the questionnaire. The second section is comprised of 24 questions, each with a set of five possible responses: “I don’t know,” “never,” “occasionally,” “sometimes,” or “always.” Scoring is the sum of the responses of the 24 questions with a score of 0 assigned for “never” and “I don’t know,” 1 for “occasionally,” 2 for “sometimes,” and 3 for “always.” This results in an overall score ranging from 0 to 72, with scores greater than 18 indicating that it is likely that the child has a sleep problem. The total score can also be broken into four sub-group scores: bedtime problems (Q1–Q6), sleep breathing and unstable sleep (Q7–Q12), parasomnia and sleep movement (Q13–Q18), and daytime problems (Q19–Q24).
Morningness Eveningness Scale for Children (MESC)
Chronotype (morning, intermediate, or evening type) of the adolescents was determined with the Chinese version of MESC [19]. The MESC is a 10-item instrument with higher scores indicating morning type. The test-retest reliability is 0.75 [19]. Per Mateo et al. [20], we assigned the upper and lower quartiles to morning- and evening-types, respectively (10–23 evening type, 24–28 intermediate type, 29–43 morning type).
Data Analysis
Internal consistency reliability, EFA, and criterion validity were analyzed by SPSS 20.0 (IBM Corp., Armonk, NY, USA). CFA was analyzed by AMOS 24.0 (IBM Corp.). The Cronbach’s α for overall score and subscale scores was estimated for internal consistency reliability. The Cronbach’s α ≥ 0.7 meant the reliability was at least acceptable [21]. The Kaiser-Meyer-Olkin (KMO) statistic and Bartlett’s test were estimated for EFA. A KMO ≥ 0.6 means the factor analysis is useful [22]. Independent samples t-tests were applied for criterion validity. Multiple goodness-offit indices were estimated for CFA, including χ2/df, Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index, Tucker-Lewis Index, and Standardized Root Mean square Residual [23,24]. Effect sizes [partial eta-squared, η2; weak (0.01 ≤ η2 < 0.059), moderate (0.059 ≤ η2 < 0.138), strong (η2 ≥ 0.138)] are reported for comparisons between chronotype and sleep problems.
RESULTS
From an initial group of Taiwanese teens (n = 497), we randomly assorted them into two groups, one to analyze for internal consistency reliability and EFA (stage 1, n = 241 parents) and one to analyze for criterion validity and CFA (stage 2, n = 256 parent/child dyads).
Internal Consistency Reliability
The reliability of the overall scale is α = 0.85 and the reliabilities of the subscales are 0.84 (bedtime problems), 0.85 (sleep breathing and unstable sleep), 0.89 (parasomnia and sleep movement), and 0.85 (daytime problems).
EFA
Factor structure was extracted by the principal components analysis with the varimax method. The KMO value is 0.81, and the Bartlett’s test of sphericity is 3239.91 (p < 0.001). The four factors extract 60% of the total variance.
Criterion Validity
Consistent with previous literature, evening-type adolescents had more sleep problems than morning types, across both the total score and each of the subscale scores of the CCASC-P (Table 1).

CCASC-P overall and subscores–comparison by chronotype
CFA
The five different summary metrics of the CFA model of the CCASC-P indicated that there was a good fit to the data (Table 2, Fig. 1).
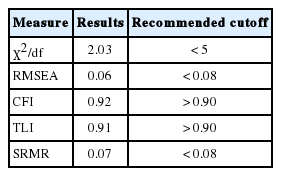
Results of the confirmatory factor analysis
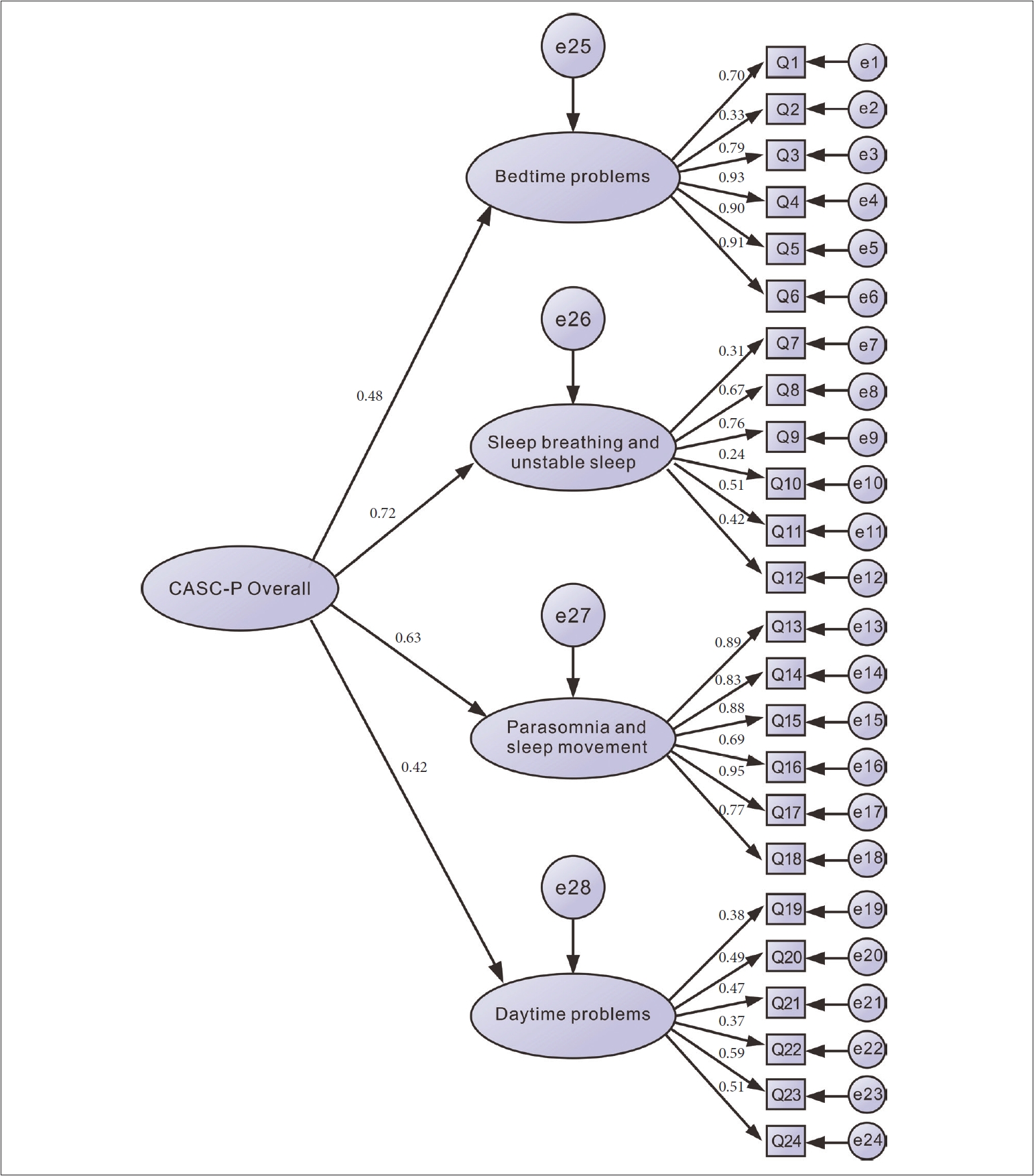
Confirmatory factor analysis of the Chinese language version of Child and Adolescent Sleep Checklist has three versions: parent/caregiver.
DISCUSSION
We found that our Chinese language translation of the CASC-P (Supplementary Materials 1 in the online-only Data Supplement) demonstrates satisfactory criterion validity as assessed by exploratory and CFA. The CCASC-P has satisfactory internal consistency (Cronbach’s alpha = 0.85), similar to that observed in the original CASC-P (Cronbach’s alpha = 0.89) [12]. CFA identified the same four factors as the original CASC-P and indicated that these reflect separate yet conceptually related constructs. No items from the original CASC-P scale were removed, indicating that the scales have similar psychometric properties for different populations. Our data indicate that the CCASC-P would be a suitable questionnaire to use to assess a parent’s perspective on adolescent sleep behavior.
The study is not without limitations. The sample included only healthy students, so the utility of the CCASC-P to examine a parent’s perspective of sleep behavior in a clinical population was not examined, nor was the association between the CCASC-P and adolescent-reported sleep behaviors. While we provide initial criterion validity to the questionnaire through examination of the association between sleep behaviors and chronotype, further research must be done to provide greater criterion validity to the questionnaire. Examination of this questionnaire in well-phenotyped clinical populations would be a necessary next step. We also did not have extensive demographic information about the parents. While we do not anticipate that the psychometric properties of the questionnaire would vary with parent gender, gender match with the child, or the age of the parent, these are possible and should be explored in future studies.
As a parent’s perception of their child’s sleep behavior may influence that child’s sleep [6], it is important to be able to accurately assess this perspective. Given the ubiquitous nature of insufficient sleep among teens worldwide, valid translations of such tools are necessary. Our study has demonstrated that the CCASC-P may be a useful tool to be used in future studies examining parental perceptions of their child’s sleep, a critical first step in improving the sleep of children.
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.17241/smr.2020.00710.
Acknowledgments
We would like to sincerely thank Chih-Chan Cheng from the Innovative Digital Content Research Center of the National Cheng Kung University who provided statistical expertise.
This study was supported by the Ministry of Science and Technology, Taiwan, R.O.C. [grant #106-2918-I-006-002, YTY].
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: Yang YT, Zeitzer JM. Data curation: Yang YT. Formal analysis: Zeitzer JM. Funding acquisition: Yang YT. Investigation: Yang YT, Zeitzer JM. Methodology: Zeitzer JM, Yang YT. Project administration: Yang YT. Validation: Hsu CY, Lin CY. Visualization: Chang HY. Writing—original draft: Chang HY, Yang YT. Writing—review & editing: Zeitzer JM, Yang YT.