Four Weeks Exercise in Obstructive Sleep Apnea Syndrome Patient with Type 2 Diabetes Mellitus and without Continuous Positive Airway Pressure Treatment: A Case Report
Article information

Abstract
The purpose of this study was to investigate the effect of exercise in patient with obstructive sleep apnea syndrome (OSAS) and type 2 diabetes mellitus (T2DM) and without continuous positive airway pressure therapy (CPAP) treatment, in polysomnography and cardiopulmonary exercise testing (CPET) parameters. 41 years old man with T2DM underwent full overnight polysomnography (PSG) and 48 hours after PSG performed maximal CPET. Patient re-checked after 24 and 28 weeks. After the 24 weeks follow-up the patient underwent 4 weeks aerobic exercise. The results showed changes between baseline and after 4 week exercise in parameters of polysomnography study, blood test and cardiopulmonary exercise testing. The findings of our study suggest that exercise can reduced the apnea-hypopnea index, improve the sleep quality and reduced the hemoglobin A1-c levels in patients with OSAS and without CPAP treatment.
INTRODUCTION
Patients with obstructive sleep apnea syndrome (OSAS) exhibit lower aerobic and anaerobic threshold capacity during cardiopulmonary exercise testing (CPET) due to the pathophysiology of OSAS patients, including lower sleep quality that causes disturbed exercise responses [1]. Moreover, OSAS patients experienced increased systolic and diastolic blood pressure during exercise due to cardiac dysfunction, decreased muscle metabolism, chronic hyper-activation of the sympathetic nervous system, and endothelial dysfunction [2]. According to Malik et al. [3], a substantial proportion of patients with type 2 diabetes mellitus (T2DM) suffer from unrecognized OSAS and conversely. T2DM is more prevalent among OSAS patients compared to those without OSAS and the treatment with continuous positive airway pressure therapy (CPAP) reduces HbA1c in a significant number of diabetics [3]. In patients with established T2DM there is a significant relationship between sleep-disorders breathing and fasting insulin, glucose, and HbA1c levels without however being aware of the exact pathophysiological mechanism linking OSAS as a causative factor of T2DM [4].
The effect of moderate aerobic exercise is similar whether the physical activity is performed in a single session or multiple bouts with the same total duration [5]. During brief, intense aerobic exercise, plasma catecholamine levels rise markedly, driving a major increase in glucose production [6]. According to Colberg et al. [5] hyperglycemia can result from such activity and persist for up to 1–2 h-1, likely because plasma catecholamine levels and glucose production do not return to normal immediately with cessation of the activity. The high-intensity interval training promotes rapid enhancement of skeletal muscle oxidative capacity, insulin sensitivity, and glycemic control in adults with type 2 diabetes [7].
The aim of this study was to investigate the effect of exercise in patient with OSAS and T2DM and without CPAP treatment, in polysomnography and CPET parameters.
METHODS
Study Design and Subject
41 years old man, uninsured due to financial crisis, with type 2 diabetes mellitus underwent full overnight polysomnography (PSG) in the Laboratory of Sleep Disorders (University of Thessaly) for suspected OSAS and 48 hours after PSG performed maximal CPET. Patient re-checked after 24 and 28 weeks (Table 1). After the 24 weeks follow-up the patient underwent 4 weeks exercise (Table 2) in Laboratory of Ergospirometry and Pulmonary Rehabilitation (University of Thessaly). Each training sessions were supervised by a pulmonologist and clinical exercise physiologist. The study was approved by the Institutional Ethics Committee and informed consent was obtained from the participant (No. of Ethical Committee 21/09-01-2017, University of Thessaly).

Data collection procedures

12 days exercise program
Data Collections
Polysomnographic recording was performed using Alice 6 (Philips, Netherlands). PSG included electroencephalography, electrooculography, submental electromyography, anteriortibialis electromyography, nasal cannula airflow signal using a nasal cannula/pressure transducer system, oral thermistor, electrocardiography, and body position. Respiratory efforts were monitored with abdominal and thoracic bands. Arterial SaO2 was measured using SpO2. Sleep was scored manually according to the criteria of Kales and Rechtschaffen [8]. Apneas were classified as obstructive, central, or mixed according to the presence or absence of respiratory efforts. A venous blood sample was collected from participant under fasting condition. Ηematocrit (Htc), hemoglobin A1c (HbA1-c), high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and gamma-glutamyltransferase were measured using standard laboratory methods. The participant 48 hours after to PSG study were subjected to ergospirometry (electronic cycle ergometer, Ergoselect 100, Ergoline, Germany) [9] until exhausting. Prior to ergospirometry were recorded the anthropometric characteristics, performed pulmonary function test [forced expiratory volume in 1st s (FEV1), forced vital capacity (FVC) and peak expiratory force (PEF) (VIASYS Health Care, Hoechberg, Germany)] [10] and estimated the strength of inspiratory (PImax) and expiratory muscles (PEmax) (MicroRPM, Care Fusion, CA, USA) [11]. The ergospirometry trial was terminated when reached symptom limited maximum exercise (respiratory exchange ratio > 1.10, HR ≥ 80% of predicted HRmax, and/or plateau of oxygen consumption with increasing work load) according to American Thoracic Society (ATS)/American College of Chest Physicians (ACCP) [12]. During 4 weeks exercise program (12 sessions) recorded before the warm-up, at the end of main set and at the end of warmdown the heart rate (HR), systolic blood pressure (SBP) and diastolic blood pressure (DBP). The exercise was done on electronic cycle ergometer (E40 Tunturi, Almere, Netherlands).
RESULTS
The PSG study, blood test, respiratory and cardiopulmonary exercise testing results showed in Table 3.
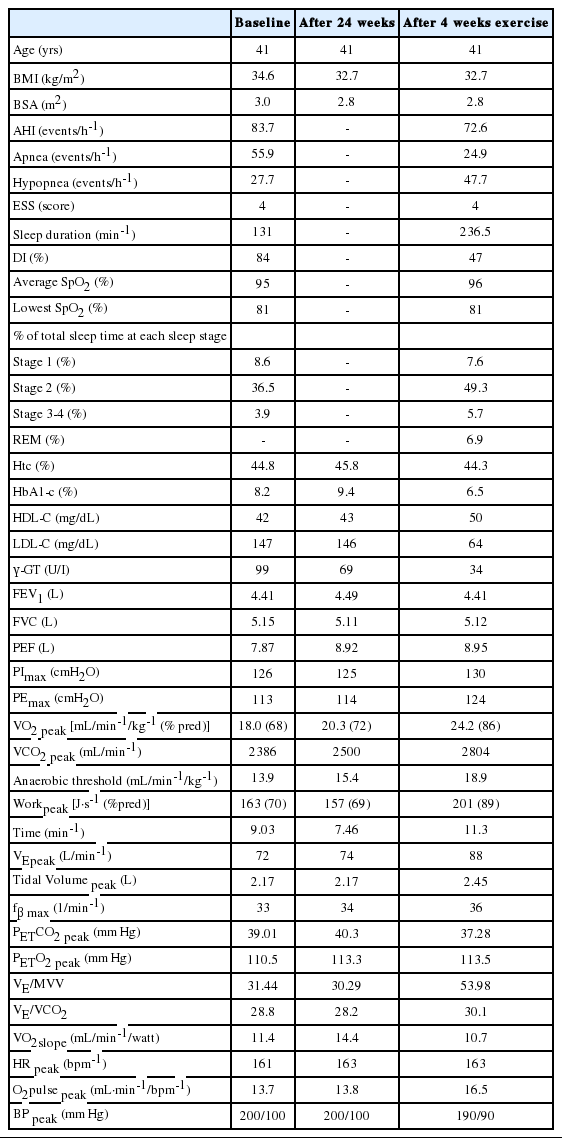
Results in polysomnography study, blood test, respiratory and cardiopulmonary exercise testing
During the sessions, the mean values of HR were before the warm-up 80 ± 7.1 bpm-1 at the end of main set 127 ± 5.6 bpm-1 and after the warm-down 99 ± 7.2 bpm-1. The mean values of SBP were before the warm-up 114 ± 4.5 mm Hg, at the end of main set 141 ± 9.4 mm Hg and after the warm-down 113 ± 4.1 mm Hg and the mean values of DBP, during the sessions, before the warm-up was 76 ± 3.8 mm Hg, at the end of mail set was 79 ± 4.5 mm Hg and after the warm-down was 71 ± 6.4 mm Hg.
DISCUSSION
The findings of our study suggest that exercise can reduced the apnea-hyponea index (AHI), improve the sleep quality and reduced the HbA1-c levels in patients with OSAS without CPAP treatment. CPAP is considered the gold standard for the treatment of sleep disordered breathing which pneumatically stabilizes the upper airways. CPAP improves glucose metabolism in patients with OSAS and T2DM and decrease further progression of the disease [13]. Moreover, the daily physical activity may have a protective role in the course of the disease [14] while patients undergoing regular exercise as treatment reduce AHI and daytime sleepiness by 32% and 28% respectively and increase VO2peak by 17.65% [15]. According to Ackel-D’Elia et al. [16], exercise training associated with CPAP treatment for OSAS patients has a positive impact on subjective daytime sleepiness, quality of life and mood state. On the other hand, many of patients do not tolerate the device CPAP thereby interrupting therapy and other patients are financially weak to buy the CPAP. However, just the exercise can not reduce it ΑΗΙ, but the exercise in OSAS patients is a low-cost treatment and should be integrated as a complementary CPAP treatment. The OSAS patients it should be encouraging participating in exercise programs so that they will decrease the cardiovascular risk, increasing the cardiopulmonary capacity and the quality of life.
Acknowledgements
The authors appreciate the friendly cooperation the participant patient.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: Stavrou V. Data curation: Stavrou V, Karetsi E. Formal analysis: Stavrou V, Karetsi E. Methodology: Stavrou V, Karetsi E. Project administration: Gourgoulianis K. Supervision: Karetsi E. Writing—original draft: Stavrou V. Writing—review & editing: Stavrou V, Karetsi E, Daniil Z, Gourgoulianis K.