INTRODUCTION
Waketime procrastination (WP) can be defined as the delay in getting out of bed in the morning after waking up. Previous studies have identified this as a problematic form of sleep behavior, particularly with regards to insomnia. For instance, it is common for individuals with insomnia to stay in bed longer than those without insomnia in the hopes of catching more sleep [1]. Most studies with insomnia patients have only focused on reducing sleep onset latency (SOL) and wake after sleep onset (WASO) [2], but relatively little attention has been given to WP.
Insomnia patients often experience early morning awakenings, and may show WP because they may try to stay in bed longer in the morning to make up for insufficient sleep. However, there is not enough research on WP from the perspective of procrastination and related psychological variables such as depression.
Insomnia and depression are highly comorbid, with about 40% of depressed patients reporting insomnia symptoms [3,4]. One common pattern of behavior observed in both of these two conditions is long periods of time spent in bed [1,5,6]. Previous studies have suggested that WP is associated with depression, as depressed people having a tendency to use the bed as an escape to solve affective problems, and stay in bed longer than less depressed people [5–7]. As such, WP is a useful behavior that requires further study in the context of depression. However, there has been a lack of direct empirical studies investigating the relationship between WP and depression.
Previous studies have indicated that it is necessary to explore sleep behaviors on weekdays and weekends separately because it is common for insomnia patients to exhibit different sleeping patterns on weekdays vs. weekends [8] which may be reflected in WP. In particular, WP may be more pronounced on weekends, when an individual may have more time to stay in bed and attempt to compensate for sleep loss without having negative consequences on their work or school.
Furthermore, gender differences in insomnia and depression patients are common [9–12]. Problematic sleep patterns associated with insomnia are typically more pronounced in women compared to men [12]. According to previous studies, women have longer SOL and WASO than men, which implies that women may be more likely to spend more time in bed (TIB) awake compared to men [13]. Additionally, it is common for gender differences to be observed in terms of coping behavior related to depression [9]. Men tend to prefer avoidant coping such as physical activity to relieve depression, while women tend to ruminate on the causes and implications of their depression [14]. This suggests that women may be more likely to cope with their depression (e.g., ruminate) in bed compared to men, hence displaying increased WP. These observations suggest that WP associated with insomnia and depression may be more pronounced in women.
Thus, the current study aims to investigate the relationship between WP, depression, and sleep in insomnia patients while considering weekend and weekday differences. We aimed to investigate the moderating effect of gender on the relationship between depression and WP according to weekdays and weekends.
METHODS
Participants and Procedures
Participants consisted of 78 adults (men = 52.6%, women = 47.4%), ranging in age from 20 to 49 years old. All participants were insomnia patients who met DSM-5 diagnostic criteria. Exclusion criteria were individuals with 1) history of psychosis, 2) suicide attempts, 3) shift workers, and 4) individuals who were currently receiving pharmacotherapy or psychotherapy for insomnia. The subjects were recruited through online advertisements in the community. All participants underwent phone screening and were scheduled for an in-person laboratory visit if eligible. During the laboratory visit, all participants completed questionnaires, and received education about completing sleep diaries. Data for sleep diaries were collected online for 7 days. This study was approved by the Institutional Review Board ethics committee (IRB number: SSWUIRB 2017-073).
Measures
Demographic information
Demographic information was collected from participants, including their gender and age.
Sleep diary
Participants completed a daily sleep diary for 7 days. Sleep diaries provide daily subjective estimate parameters about sleep, including bed time, SOL, frequency of nocturnal awakenings, WASO, wake time (WT), time out of bed, feeling upon arising and sleep quality. WP was derived from the sleep diary, and was operationally defined as the time spent from WT to time out of bed. TIB (the length of time spent in bed), total sleep time (TST; total time spent asleep), and sleep efficiency (SE; ratio of TST to TIB multiplied by 100%) were also calculated based on sleep diary parameters.
Korean version of Center for Epidemiologic Studies Depression Scale Revised
The CESD scale was developed to measure severity of depression symptom [15]. The Korean version of Center for Epidemiologic Studies Depression Scale Revised (K-CESD-R) is a 20-item self-report questionnaire that evaluates the severity of depression symptom [16]. Subjects respond to the degree they have experienced depression symptoms in the past week and how often they experience depression symptoms during the week. Each of the K-CESD-R items are scored on a 5-point Likert scale ranging from 0–4. Total scores range from 0 to 80, with higher scores reflecting higher symptomatology [17]. According to Van Dam and Earleywine [18], a cut off score of 16 is recommended to determine clinical levels of depression. Cronbach’s α of the K-CESD-R in this sample was 0.914.
Insomnia Severity Index
Insomnia Severity Index (ISI) is a 7 item self-report questionnaire that evaluates the severity of insomnia, each of items include factors that difficulty falling asleep and staying asleep, problems waking up to early, satisfaction with current sleep patterns and difficulty with daily functions etc. Each of ISI items are scored on a 5-point Likert scale, rating on a scale of 0 to 4. A total score is calculated by summing up all items, ranging from 0 to 28. In ISI, the higher scores indicate more severe insomnia [17]. Cronbach’s α of the ISI in this sample was 0.640.
Statistical Analyses
All statistical analyses were conducted by using SPSS Statistics version 21 (IBM Corp., Armonk, NY, USA). All parameters were calculated separately for weekdays and weekends. Correlational analyses were conducted using Pearson’s correlation coefficient between sleep variables and clinical indicators. T-tests were conducted to determine gender differences in WP and other variables. Some variables were analyzed with non-parametric analysis because they did not meet normality assumptions (Mann-Whitney test). Moderation analysis was conducted by using SPSS Process Macro (A Division of Guilford Publications Inc., New York, NY, USA). We examined the moderating effect of gender on the relationship between depression and WP after adjusting for insomnia severity. For verifying data analysis, we used bootstrapping that was proposed by Shrout and Bolger [19]. Using this model, the relationship is interpreted as statistically significant if the 95% confidence interval of the repeated sample does not include zero.
RESULTS
Gender Differences in Sleep and Depression
General characteristics of the sample are shown in Table 1. Table 1 presents gender differences for sleep and clinical variables. Sleep variables are presented separately for weekdays and weekends. Gender differences for WP were significant on weekdays (p = 0.003) and weekends (p = 0.034). Women engaged in more WP than men during both weekdays and weekends. Both women and men engaged in more WP on weekends than on weekdays.
There was a significant gender difference for severity of depression (p = 0.016), with women reporting feeling more depressed than men. There were also gender differences for SOL, TIB, and SE, which was significant for both weekdays [SOL (p < 0.001), TIB (p = 0.006), SE (p < 0.001)] and weekends [SOL (p = 0.039), TIB (p = 0.038), SE (p = 0.003)]. Women took longer to fall asleep than men during both weekdays and weekends and spent more TIB, and had lower SE compared to men. The gender difference for WT on weekdays (p = 0.157) and weekends (p = 0.224) was not significant. In our study, 60 people woke up earlier than planned on weekdays, and 48 on weekends.
Association between WP, Sleep, and Depression
Table 2 presents the correlations between WP, sleep variables (WT, SOL, WASO, TST, TIB, SE), and depression (K-CESD-R). WP was significantly positively correlated with depression scores on both weekdays and weekends (ps < 0.01). Thus, higher levels of WP on weekdays and weekends were associated with more depression symptoms.
Moderating Effect of Gender on the Depression-WP Relationship based on Weekdays and Weekends
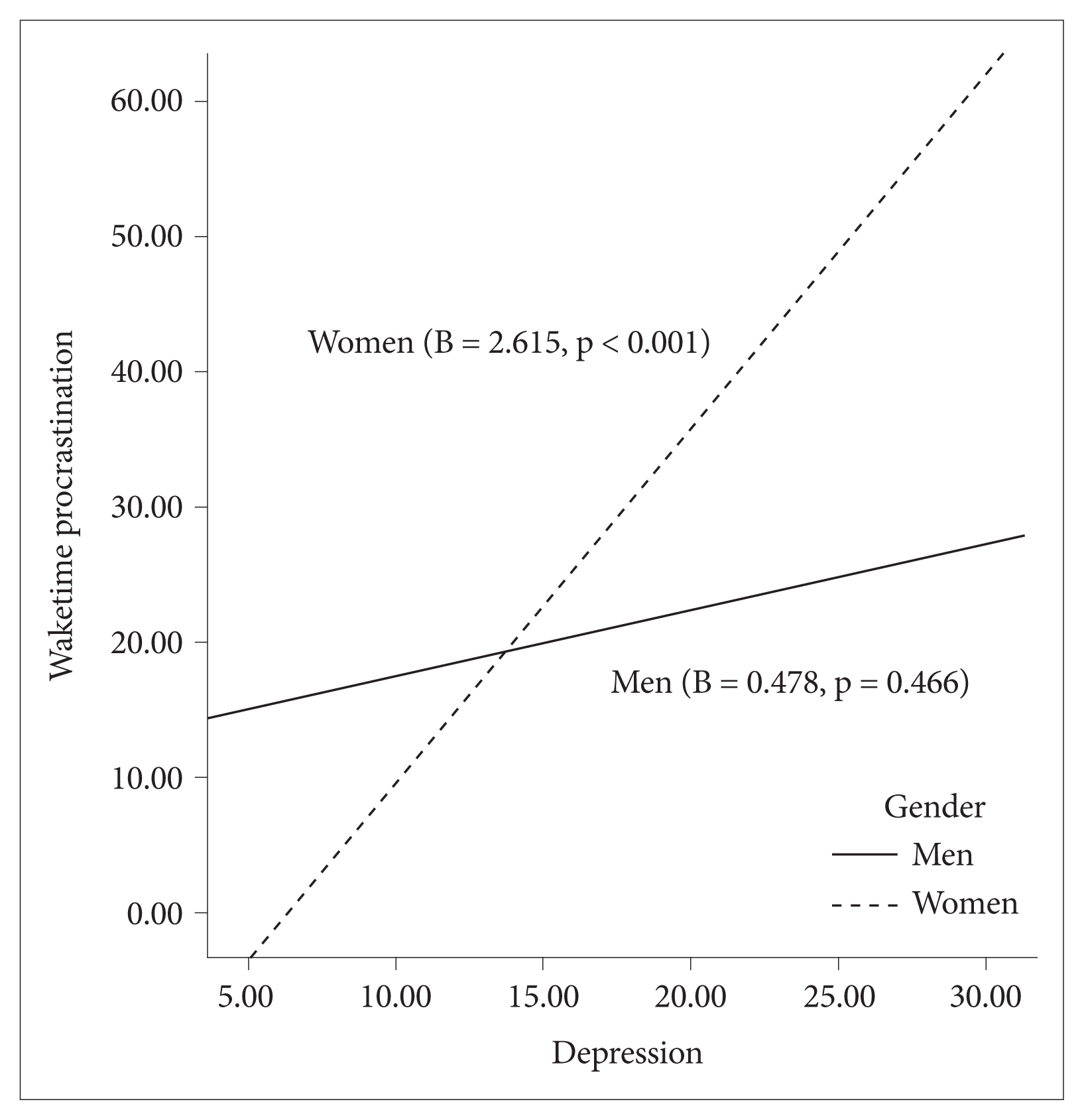
Results for the moderator analyses are shown in Table 3. On weekdays, results indicated that there was a significant main effect for depression (B = 1.298, p < 0.001) and gender (B = 30.108, p = 0.002). Gender had a moderating effect on the relationship between depression and WP (B = −1.239, p = 0.005). Meanwhile, on weekends, the main effect for depression (B = 0.478, p = 0.466) and gender (B = −29.456, p = 0.079) were not significant. However, there was a significant moderating effect of gender on the relationship between depression and WP (B = 2.136, p = 0.006).
To test the effect size of the moderating variables, we confirmed that gender was a moderator using bootstrapping. Through confirming to effect of depression severity on WP depending on gender differences, we tested the significance of the interaction effect (Table 3). On weekdays, the moderating effect was significant for men (B = 1.298, SE = 0.373, t = 3.481, p < 0.001), but not for women (B = 0.059, SE = 0.283, t = 0.209, p = 0.835). On weekends, meanwhile, the moderating effect was not significant for men (B = 0.478, SE = 0.653, t = 0.732, p = 0.466), but significant for women (B = 2.615, SE = 0.495, t = 5.280, p < 0.001). These results suggest that for men, the more depressed they were on weekdays, the more they engaged in WP. In contrast, on weekends, the more depressed that women felt, the more they engaged in WP. These results are presented in Figs. 1 and 2.
DISCUSSION
The main finding of this study was that WP was related to depression and that individuals with high levels of depression engaged in more WP than their non-depressed counterparts. Women reported more WP than men on both weekdays and weekends. When men did engage in WP, they reported more WP on weekends than weekdays. Only men with high depression showed significantly more WP on weekdays, while only women with high depression showed significantly more WP on weekends. To the best of our knowledge, this is the first study investigating WP in the context of insomnia and depression considering gender differences.
Waketime Procrastination and Depression
Our study found that higher levels of depression was associated with higher levels of WP in insomnia patients; this was consistent with previous studies reporting that depressed people spend prolonged TIB [5–7,20,21]. WP may be a behavior that indicates low motivation levels among major depression disorder patients. Depressed people often complain of reduced energy levels and feelings of helplessness, which often makes it difficult to get ready for work in the morning [6,7,21,22]. Low levels of motivation in depressed people can also be found in neuroimaging studies. People with depression have decreased serotonin in the ventromedial prefrontal cortex, and dopamine deficiency is observed due to abnormal activity in the ventral striatum, which has been associated with procrastination, and lack of motivation [23,24]. Therefore, low mood and lack of motivation, especially in the morning, may cause depressed people to have difficulty getting out of bed in the morning.
It is well known that patients with severe depression feel depressed in the mornings and gradually improve as the day progresses [25]. According to Lemke’s study [26], patients with depression reported significantly higher levels of depression in the morning. Healthy people experienced a decrease in depression after getting sufficient sleep, but sleep disturbance may exacerbate depression symptoms. This is thought to be caused by qualitative differences in sleep patterns of depressed people. Therefore, depressed people can feel more depressed in the morning after sleeping [27]. In fact, depressed patients have lower blood thyroxin levels in the morning, which is associated with a depressed mood. According to one study, patients with depression had lower levels of Vanilmandelate and Homovalilate in their urine in the morning compared to in the evening, which was related to lower thyroxin levels [28].
The Moderating Effect of Gender in the Relationship between WP and Depression on Weekdays and Weekends
In this study, although gender differences for WT was not significant, women had more WP than men, which may be due to gender differences in depression that are reflected in WP. Gender differences in depression are widely known, and women generally report a higher level of depression than men [30]. In this study, gender moderated the relationship between depression and WP. In our study, depressed men reported more WP on weekdays than women, which suggests that depression in men may mainly be a reflection of social withdrawal [31]. Generally, there are social schedules such as work and school during weekdays, and the severity of depression in men may lead to prolonged WP in order to delay starting these social schedules during the weekdays. Meanwhile, the same effect was not found on weekends for men, which may be related to the characteristics of coping styles for depression more likely in men. Studies have reported that men are more likely to choose active coping strategies to alleviate a depressed mood compared to women [14]. This suggests that on weekends when there are limited social schedules, depressed men are likely to get out of bed in order to actively cope with their depressed mood.
Women reported more WP on weekends, but the effect was not significant during weekdays. Rumination is a major predictor of depression, and women use rumination more often than men to cope with depression [9,32]. Depressed people tend to use the bed as escape to cope with their depression, and from a behavioral perspective, rumination helps depressed individuals avoid the aversive environment surrounding them [7,9]. Also, depressed women tend to complain more about fatigue and physical pain than depressed men [33,34].
This is the first published study to explore gender differences in the relationship between WP and depression. While it is widely known that staying in bed for prolonged periods of time is associated with depression and insomnia, previous sleep studies have focused on pre-sleeping behavior (such as bedtime procrastination) and have overlooked WP. In this study, we investigated gender differences in the relationship between WP and depression and suggest the need for interventions for WP in the sleep treatment of insomniac patients with depression.
The relationship between depression and WP may differ based on gender and weekdays and weekends differences. For example, individuals are generally more stressed due to their job during weekdays than on the weekend, and this stress has been identified as a trigger for depressive symptoms in men [35]. Based on the literature, psychosocial factors such as financial and professional failure are especially high-risk factors for depression among men [30]. This suggests that they may experience more depressive symptoms than women during the weekdays, thus depression in men may be reflected by greater WP during weekdays than women. In addition, there is more opportunity for individuals to cope with their emotions on the weekends [36]. In coping with depression, women prefer less active solutions than men [14], indicating that depressed women may exhibit higher WP than depressed men on the weekends.
In our study, both men and women reported more WP on weekends than weekdays; this is consistent with the hypothesis of this study that WP is more likely to occur on weekends when there are less required social schedules. In general, people lie in bed longer on weekends than on weekdays [37], and previous studies have reported that deviations in sleep patterns during weekends compared to weekdays have a negative effect on sleep and mood [38]. Extending this view, our study suggests that weekday-weekend differences in WP may also negatively affect an individual’s sleep and emotions.
Clinical Implications
In general, cognitive behavior therapy for insomnia uses behavioral techniques such as sleep restriction and stimulation control, but often does not directly assess or provide interventions specifically targeting WP. In this study, WP was measured using a 7-day sleep diary utilizing the difference between WT and time out of bed. This is a sleep parameter that is not often used to guide treatment in most behavioral interventions for insomnia or depressed individuals. Our study found gender differences in WP, which is generally consistent with where women report more insomnia, and emphasized the importance of therapeutic interventions tailored to gender [11]. Insomnia patients who have long WP should also be screened for depression. Also, clinicians can check their lifestyle or activities and recommend the better coping strategies based on gender.
Limitation
This study was an exploratory study of gender differences in the relationship between WP and depression in a clinical group with insomnia. This study relies on subjective reports of sleep and depression. Further studies using objective measures of sleep (e.g., polysomnography and actigraphy) and biological indicators of depression (e.g., fMRI) may provide more information as to why depression is associated with high levels of WP. Second, the current study was a cross-sectional study investigating WP. These observations suggest that WP associated with insomnia and depression may be more pronounced in women. In future research, it is necessary to explore psychological mechanisms of WP through longitudinal studies. Third, this study did not collect information about employment, years of education, marital status, parental status, and cohabitation, which may have been helpful in identifying the population. Fourth, since this study did not examine coping styles, there may be limitations in interpreting the effects of gender. Finally, this study is limited to a relatively young age group (20–40 age range). Age has been shown to be significantly associated with a bigger discrepancy between weekday and weekends due to stronger eveningness tendency [39,40]. Thus, future studies may need to replicate the relationship between WP and depression in an older age group.
Conclusion
This study investigated gender differences in the relationship between WP and depression in an insomniac group. High levels of depression were associated with high levels of WP. Men with high depression showed more WP on weekdays and women with high depression showed more WP on weekends. WP is often overlooked in sleep studies and treatment; our study suggests that WP is an important behavior to consider in the clinical context of providing sleep therapy to depressed individuals, particularly while taking gender differences into account.