INTRODUCTION
The importance of sleep in physical and mental well-being is generally acknowledged by both health professionals and the general public. Sleep apnea has been increasingly recognized as a potential cardiovascular risk factor. Initial physiological-based studies demonstrating acute effects on cardiovascular physiology during sleep have been followed by prospective epidemiological studies that supported the longitudinal association with cardiovascular disease (CVD). The aim of this review is to summarize major evidence accumulated and discuss future investigations under development in sleep and CVD. While the major focus will be on sleep apnea, other aspects of sleep will also be highlighted.
Pathophysiology of Sleep Apnea’s Impact on Cardiovascular System
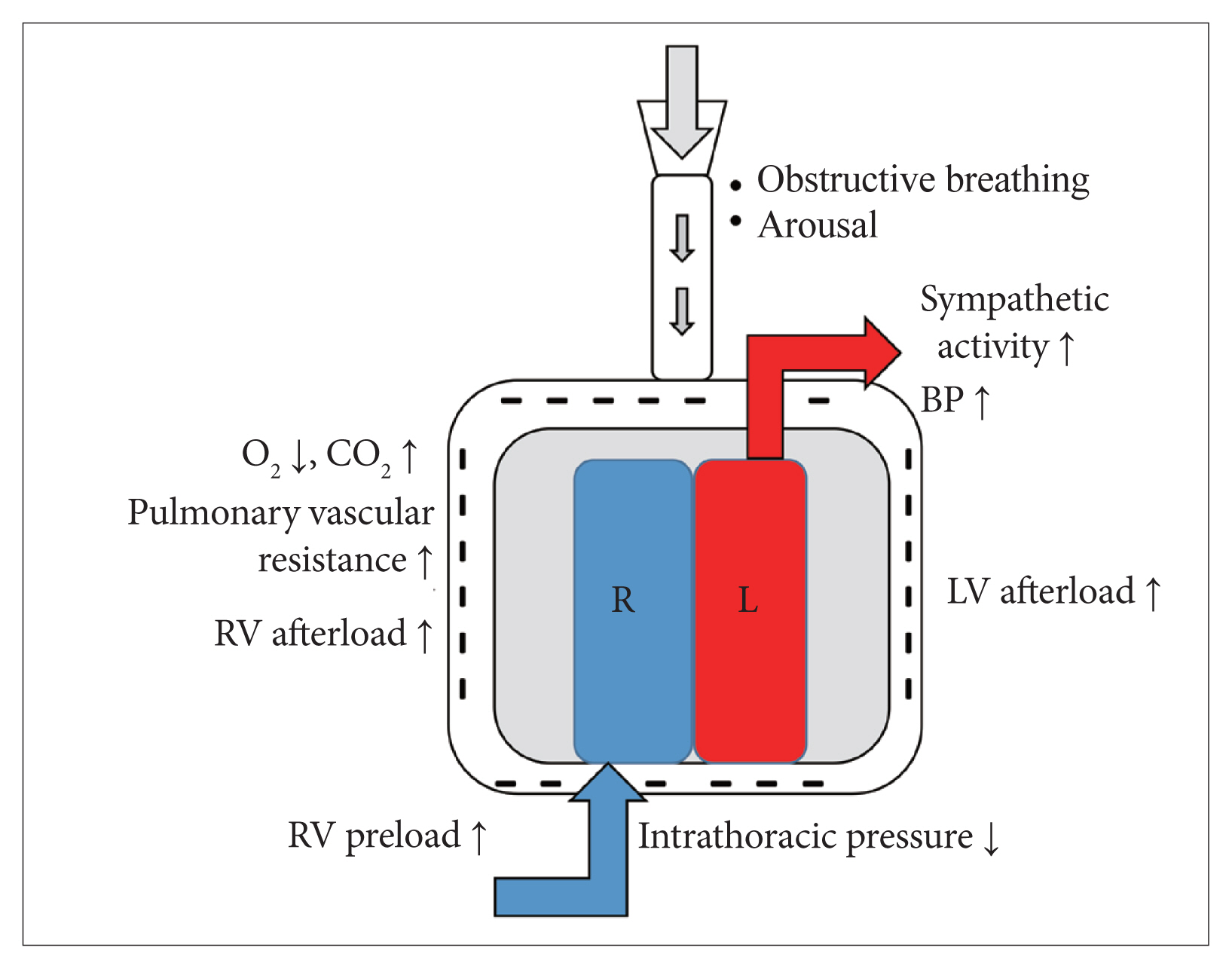
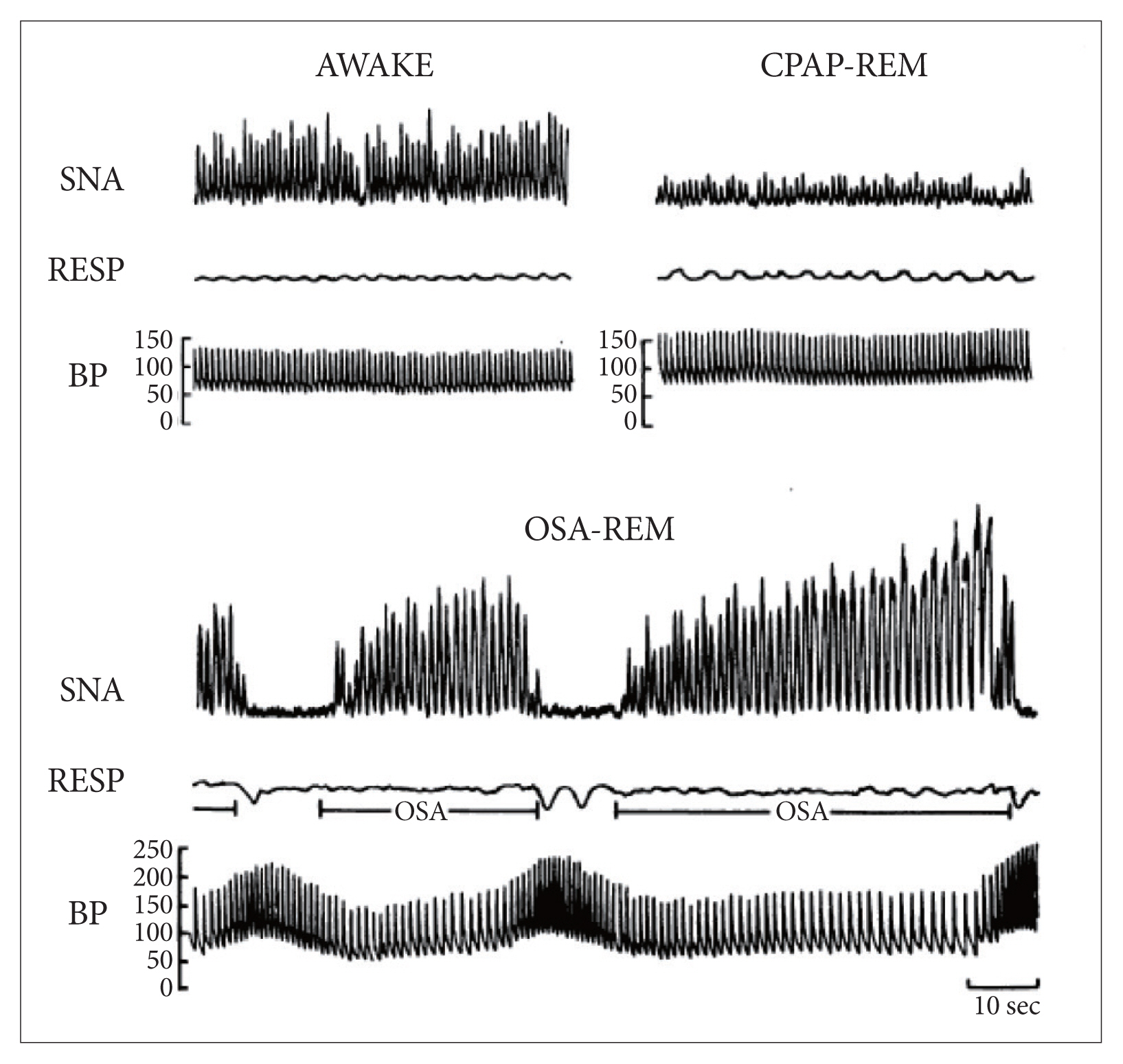
Obstructive sleep apnea (OSA) is defined by recurrent episodes of upper airway obstruction during sleep. In addition to upper airway anatomy, impairment of neuromodulatory control of the upper airway muscles during sleep plays an important role in the pathogenesis of OSA [1]. Repetitive forceful inspiration against a closed airway generates intrathoracic pressure swings, which in turn can increase left ventricular transmural pressure (Fig. 1) [2,3]. The resulting surges in sympathetic tone increases arterial stiffness and blood pressure (BP) (Fig. 2) [4]. Persistence of high sympathetic tone carried over to the hours spent awake may be an important mechanism of OSA-associated hypertension. Cessation of breathing leads to gas exchange abnormalities characterized by intermittent hypoxemia and hypercapnia-another important cause of increased sympathetic tone. Chronic intermittent hypoxemia is likely critical in ex plaining many cardiovascular and metabolic consequences of OSA [5]. Moreover, the obstructive events frequently culminate in arousals, thereby disrupting sleep continuity and contributes to some of the symptoms of OSA such as non-restorative sleep and daytime sleepiness.
Sleep Apnea and Hypertension
The association between OSA and hypertension has been widely studied, and OSA has been established as an independent risk factor for hypertension (the Joint National Committee-7). Obstructive respiratory events leading to sympathetic surges are accompanied by varying degrees of acute elevation in BP. In fact, OSA is believed to be an important cause of non-dipping (lack of an appropriate decrease in BP that normally occurs in sleep). In addition to this nocturnal (more accurately “asleep”) hypertension, OSA is also associated with daytime hypertension. A significant proportion of patients with resistant hypertension have concomitant OSA [6]. The Wisconsin cohort study, a landmark prospective cohort study, demonstrated a dose-response relationship between severity of OSA and risk of incident hypertension [7]. Subsequent prospective data from the Sleep Heart Health Study (SHHS) demonstrated a similar dose-response relationship between OSA and hypertension, though this was largely attenuated after adjusting for body mass index [8]. Indeed, hypertension is a component of the STOP-BANG Questionnaire, a commonly used OSA risk assessment tool [9]. Effective treatment of OSA with continuous positive airway pressure (CPAP) has been shown to improve long-term BP control based on 24-hour ambulatory BP monitoring [10]. While there is some conflicting data, the literature overall shows that CPAP improves BP control, particularly among patients with resistant hypertension [11,12]. Considering the high prevalence of OSA and the adverse consequences of both daytime and nocturnal hypertension on cardiovascular outcomes, identification, and the treatment of OSA among patients with hypertension has important public health implications.
Sleep Apnea and Atrial Fibrillation
Atrial fibrillation (AF) is one of the most prevalent chronic arrhythmias, affecting millions in the United States. The rise in its prevalence is partly attributed to a rapidly aging population [13], but ongoing efforts are being made to identify novel and potentially modifiable risk factors for AF. OSA is highly common in patients with AF. Moreover, the relative risk of having nocturnal AF was found to be markedly higher in people with severe sleep apnea in the SHHS [14]. However, association between the prevalence of sleep apnea and AF (beyond nocturnal AF) in unselected populations from the community remains uncertain. In the multi-ethnic study of atherosclerosis, the prevalence of AF increased according to the severity of OSA. Moreover, there is evidence that OSA plays a role in the recurrence of AF following catheter-based AF ablation, while treatment of OSA with CPAP appears to reduce the risk [15,16]. However, such findings have not been replicated in other observational studies, reflecting some degree of uncertainty as to whether OSA truly contributes to post-ablation AF recurrence [17,18]. While awaiting results from several ongoing randomized controlled trials (RCTs) on this issue, screening and treatment of OSA in the presence of sleep-related symptoms seems reasonable [19]. Future studies are warranted to identify high-risk groups for incident or recurrent AF among patients with OSA [20]. For example, it is possible that patients with OSA with either electrographic or structural left atrial pathology may be at much higher risk for developing AF [21–23]. Such information can help to arrive at treatment decisions in patients without obvious symptoms. Additionally, other elements of sleep may play a possible role in AF. Lack of deep sleep was found to be more common in patients with AF independent of OSA [24,25]. A recent observational study showed that lack of rapid eye movement sleep is associated with an increased risk of incident AF [26]. Both subjectively reported sleep difficulty and objectively assessed short sleep duration have been linked to AF [26,27]. These findings highlight the complex interplay between sleep in its entirety and AF [20].
Sleep Apnea and Sudden Cardiac Death
Out-of-hospital sudden cardiac death (SCD) is a major cause of cardiac mortality. A limited but emerging body of research has further elaborated on the link between sleep apnea and SCD. There is a paucity of epidemiological data examining the association between OSA and SCD due to relative rarity of the event in existing sleep cohort studies. One clinic-based cohort study showed that the lowest nocturnal oxygen saturation was independently, albeit modestly, predictive of SCD in an average 5-year follow-up period [28]. However, it is plausible that the SCD could have resulted from other underlying cardiopulmonary conditions or morbid obesity, which are associated with both oxygen saturation and SCD [29]. Despite these limitations, this study represents the first of its kind to suggest OSA as a possible independent risk factor for SCD. Circadian timing of SCD may be shifted in patients OSA [30,31]. The relative risk for SCD was significantly higher between midnight and 6 a.m. in patients with OSA compared to the general population [30]. One mechanism that would explain the link is the influence of OSA on ventricular depolarization and repolarization. Patients with OSA more commonly exhibit high risk electrocardiographic markers such as prolonged QT, T peak to T end (TpTe) interval and high QRS-T angle, all of which confer high risk for malignant arrhythmias [32–34]. Although the role of OSA in SCD needs further elucidation, we speculate that OSA possibly increases the risk of SCD via increasing risks for other CVD such as coronary heart disease. Appropriate implantable cardioverter-defibrillator therapy is more common in heart failure (HF) patients with sleep apnea [both OSA and central sleep apnea (CSA)], which suggests the risk of SCD in these patients [35].
Sleep Apnea and Stroke
Sleep apnea is common in patients with stroke or transient ischemic attack (TIA) [36–39]. On the other hand, OSA appears to increase the risk of ischemic stroke. In the landmark study by Yaggi et al. [40], OSA was associated with a two-fold increased risk of stroke or death. Furthermore, there was a dose-response relationship between the severity of OSA and the risk of ischemic stroke. In the SHHS, men, but not women, in the highest quartile apnea-hypopnea index had approximately three times higher risk of ischemic stroke compared to those in the lowest quartile [41]. Aggravation of cerebrovascular abnormalities, hypertension and AF are speculated to be some of the mechanisms. In the sleep apnea cardiovascular endpoints (SAVE) trial, there was no difference in the incidence of stroke, one of the primary outcomes, between those who were randomized to CPAP vs. no CPAP [42]. In terms of CPAP effect on the outcomes among patients with stroke, a RCT is underway to test whether treatment of OSA with CPAP immediately after stroke or TIA would improve outcomes [Sleep for Stroke Management and Recovery Trial (Sleep SMART; https://clinicaltrials.gov/ct2/show/NCT03812653)].
Sleep Apnea and Coronary Artery Disease
OSA is common in patients with coronary artery disease (CAD). About one third of patients with stable CAD were noted to have OSA [43,44]. In patients with acute myocardial infarction (MI), the prevalence of OSA is even greater, with some reports citing figures as high as 66% [45]. However, severity of OSA may resolve from the acute to recovery phase following acute MI. Of the patients newly diagnosed with OSA at index admission (46%), resolution of OSA was seen in approximately half six months later [46]. Increased platelet activation and aggregation, along with endothelial dysfunction due to inflammation and oxidative stress, predispose to atherosclerotic plaque formation in OSA [47]. OSA is also associated with a higher burden and progression of coronary artery calcification, which is a potent predictor of acute MI and CVD [48,49]. More importantly, two major sleep cohort studies showed increased risk of future CAD in patients with OSA [50,51]. OSA was also found to be independently associated with a larger coronary atheroma volume, but not with necrotic core volume, based on an intravascular ultrasound with virtual histology technology in patients undergoing coronary angiogram [52]. OSA also leads to more adverse outcomes in patients undergoing percutaneous coronary intervention [53]. In the post-hoc analysis of patients with concomitant diabetes, OSA increased the risk of adverse cardiovascular events by two-fold [54]. In particular, the 3-year estimated cumulative incidence of cardiovascular mortality for patients with both OSA and diabetes over a median follow-up period of 1.9 years was 7.4%, compared to 1.4% in those with diabetes but without OSA (p = 0.002) [54]. In patients undergoing non-urgent coronary artery bypass surgery, OSA was independently associated with a nearly 5 times higher likelihood of unscheduled re-admissions due to cardiovascular events at 6-month follow-up [55]. The ultimate question is whether OSA treatment would effectively lower this increased risk of cardiovascular events. A small pilot study using hybrid positron emission tomography/magnetic resonance imaging technology with 18F-FDG tracer measured vascular inflammation in patients with OSA. The study demonstrated a decrease in carotid plaque activity in patients with good adherence to optimum CPAP therapy for a minimum period of 3 months. Quantitative analysis showed reduction of carotid and aortic plaque inflammation, comparable to outcomes achieved with statin therapy [56]. However, in the SAVE trial, CPAP therapy did not reduce cardiovascular events including acute MI [42]. In a recent RCT, OSA screening and treatment via a multidisciplinary approach (vs. no OSA screening and treatment) in patients with acute coronary syndrome did not lead to reduction in the levels of cardiovascular biomarkers such as N-terminal pro-brain natriuretic peptide, suppression of tumorigenicity 2 and high-sensitivity C-reactive protein [57]. It therefore remains uncertain whether OSA treatment improves the outcomes following acute MI.
Sleep Apnea and Heart Failure
Several epidemiological studies have suggested that sleep apnea is associated with an increased risk of incident HF [50,51, 58]. In patients with HF, sleep apnea is highly prevalent [59,60]. A unique feature of sleep apnea in patients with HF is the high prevalence of CSA (15–40%) in addition to OSA (12–53%) [60–64]. CSA typically accompanies Cheyne–Stokes breathing, a form of periodic breathing characterized by a crescendo-decrescendo pattern of hyperpnea, followed by central apnea or hypopnea. The mechanism involves instability of the respiratory control system in association with pulmonary congestion, increased chemosensitivity, and delayed circulation time [65–67]. Both OSA and CSA are associated with increased mortality in patients with HF [68,69]. Although CSA is more likely a consequence rather than a cause of HF, CSA initiates a vicious cycle that could cause further deterioration and increased mortality in HF patients [65,66,70]. Several short-term RCTs showed beneficial effects of OSA treatment with CPAP on cardiac function, such as increase in left ventricular ejection fraction (LVEF) in patients with HF [68]. Although no RCTs showed the effects of CPAP on mortality in OSA patients with HF, observational studies suggested that OSA treatment with CPAP was associated with decreased risk of mortality [68,69,71]. In patients with CSA, optimization of HF treatment should be prioritized as CSA improves with improvement in HF [65,66]. Whether suppression of CSA by itself improves the clinical outcomes is unclear. The Canadian Continuous Positive Airway Pressure for Treatment of Central Sleep Apnea in Heart Failure (CANPAP) trial showed that CPAP alleviated CSA, and improved LVEF, but failed to show mortality benefit. This could possibly be due to insufficient suppression of CSA, observed in about half of the participants in the CPAP group [72,73]. Therefore, routine use of CPAP is not supported for patients with HF and CSA, but may be used if CSA can be sufficiently suppressed by CPAP. Although CPAP may suppress CSA (possibly through cardiac unloading), CPAP is typically not very effective in treating CSA [74]. Adaptive servo-ventilation (ASV) is an advanced mode of bi-level positive airway pressure developed for the treatment of CSA [75,76]. Short-term RCTs showed beneficial effects on cardiac function in those with CSA treated by ASV [65]. However, in the Treatment of Predominant Central Sleep Apnea by ASV in Patients With Heart Failure (SERVE-HF) trial, ASV failed to show mortality benefit [77]. In addition, all-cause and cardiovascular mortalities and secondary endpoints were significantly worse in patients treated with ASV compared with the control group. Although specific reasons for this remain unknown, nonadherence to the study protocol (29% of patients in the ASV group either discontinued use of ASV or never used it, and 17% of patients in the control group crossed over to positive airway pressure therapy) may play some role. One ongoing RCT using ASV in patients with HF and CSA, a multi-centre, randomized study to assess the Effects of Adaptive Servo Ventilation on Survival and Frequency of Cardiovascular Hospital Admissions in Patients with Heart Failure and Sleep Apnea (ADVENT-HF), may shed more light on the impact of treatment of CSA with ASV [78]. Supplemental oxygen during sleep has been shown to alleviate CSA and increase the exercise capacity [79,80]. The Impact of Low Flow Nocturnal Oxygen Therapy on Hospital Admissions and Mortality in Patients With Heart Failure and Central Sleep Apnea (LOFT-HF) RCT trial is underway to assess the effectiveness of supplemental oxygen in clinical outcomes (https://clinicaltrials.gov/ct2/show/NCT03254212). Phrenic nerve stimulation is a novel option that has been shown to be effective in suppressing CSA and improving sleep, quality of life and LVEF [81–85]. RCTs are warranted to confirm clinical efficacy of phrenic nerve stimulation on HF.
Other Sleep Aspects and Cardiovascular Disease
Sleep is one of the foremost critical behavioral factors for overall health, as well as physiological processes, emotion regulation, cognitive performance, and quality of life [86]. There is a growing body of evidence supporting both abnormal sleep duration and poor sleep quality as important risk factors for CVD. Both self-reported or objectively measured short and long sleep duration have been found to be associated with subclinical and clinical CVD [27,87–95]. A meta-analysis of prospective studies including 474686 participants with 6.9–25 years of follow-up showed a U-shaped association between sleep duration and CVD, reporting that individuals with either shorter or longer sleep than 7–8 hours per night are at increased risk of CVD [96]. While this U-shaped has generally been advocated, the relation is more complex. For example, objectively measured sleep duration had a positive linear relationship with arterial stiffness in the community-dwelling elderly population [97]. Furthermore, a meta-analysis on over 3 million participants demonstrated a J-shaped relationship between sleep duration and increased risk for mortality and incident CVD [98]. Unlike subjective sleep quality, definition of objective sleep quality is more complex [99]. Increased sleep efficiency, reduced wake after sleep onset time and sufficient time spent in deep sleep (such as slow wave sleep and rapid eye movement sleep) are often used as indicators of good sleep quality [100]. Similar to sleep duration, both self-reported and objective sleep quality have been linked to subclinical and clinical CVD [24,25,101–106]. Therefore, both sleep duration and sleep quality are vital as these present as several phenotypes with varying degrees of health consequences. For example, one large cohort study showed that over 10–15 years of follow-up, short sleepers had a 15% higher risk of CVD and a 23% higher risk of CAD compared with normal sleepers. However, short sleepers with poor sleep quality had a 63% higher risk of CVD and a 79% higher risk of CAD compared with normal sleepers with good sleep quality [107]. A recent large nationwide cohort study from Taiwan reported that having a history of a non-sleep apnea disorder based on international diagnostic codes was associated with an increased risk of HF [108]. Another nationwide cohort study reported increased risk of ischemic stroke with insomnia [109]. Many existing studies looking at the interface of sleep and CVD have generally focused on a single domain of sleep (e.g., sleep apnea alone). The multidimensional nature of sleep has been overlooked. In fact, many studies examining subjective sleep duration and quality in relation to CVD lacked objective sleep studies, and studies examining sleep apnea lacked subjective sleep report, all of which are equally important. As a result, it is often difficult to fully appreciate the independent associations of individual components from these studies. Furthermore, psychological factors are known to have a major impact on both sleep and CVD [110,111]. Given behavioral mediation of the relationship between psychological factors and health outcomes, it is plausible that impaired sleep may be a critical mediator of the relationship between stress and CVD. Further studies deciphering this complex interaction between stress, sleep, and cardiovascular health are warranted.
Future Directions
A growing body of evidence has been pointing to adverse effects of sleep apnea on cardiovascular health. In symptomatic patients with sleep apnea, treatment of sleep apnea improves sleep quality and quality of life regardless of their cardiovascular risks or burden [112]. Considering the high burden of sleep apnea in patients with cardiovascular comorbidities, timely screening and treatment are important. However, there is a remaining question about whether treatment of sleep apnea improves cardiovascular-related clinical outcomes beyond the quality of life. Several ongoing RCTs may help narrow this gap. Searching for sleep study metrics and other physiological markers that would better characterize cardiovascular impact of sleep apnea and response to therapy beyond conventional respiratory-centric metrics would be highly valuable. Other areas that lack high quality evidence on the impact of sleep apnea and its treatment include pulmonary hypertension and peripheral vascular disease. In the context of primary prevention, more investigations are needed to better identify high-risk patients who may benefit from sleep apnea treatment. The common treatment modality of choice for OSA is CPAP, but it is not well accepted and tolerated by most patients. Development of cost-effective and more convenient therapies for sleep apnea is critically needed. Furthermore, the role of other aspects of sleep beyond sleep apnea in mediating the outcomes in patients with CVD warrant further investigation.